The position of the heart is systematically assessed during fetal cardiac examination. A change in heart position is uncommon and very important, as it may be associated with intracardiac and extracardiac structural anomalies.1
Mesocardia in an uncommon cardiac abnormality, in which the heart is positioned in the center of the thorax and its longitudinal axis lies in the thoracic mid-sagittal plane. The true incidence of this condition is unknown.
Mesocardia is usually associated with other structural cardiac abnormalities, but occasionally it is found alone. Most of the reported prenatal cases are related to heart defects or extracardiac anomalies. Displacement of the heart to the thoracic midline can occur secondary to an intrathoracic mass, pulmonary abnormalities, or diaphragmatic hernia.1 Mesocardia has also been described in association with severe cardiac anomalies, heterotaxy, chromosome disorders, and genetic syndromes.1,2
Here, we describe 2 cases of mesocardia diagnosed prenatally in our prenatal diagnosis unit, together with their ultrasound characteristics.
The first case was the fifth pregnancy in a 33-year-old woman whose 4 previous pregnancies had culminated in 1 birth and 3 abortions. She came to our unit for early fetal echocardiography at 16 weeks’ gestation. The fetal heart was in a midline position and showed an associated persistent left superior vena cava (LSVC). No additional cardiac or extracardiac structural abnormalities were detected. The heart showed an atypical morphology: The left ventricle had a rounded shape instead of the characteristic inverted cone, and the cardiac apex had an unusual appearance. The patient did not wish to undergo amniocentesis. There were no changes on fetal follow-up. At 36+6 weeks, a girl was born by natural vaginal delivery, with good clinical status and weighing 2230g. Mesocardia and persistent LSVC were confirmed postnatally. At the time of writing, the child is 24 months of age and she has remained asymptomatic except for 1 episode of acute bronchiolitis.
The second case was the first pregnancy in a 30-year-old woman, who attended our prenatal diagnosis unit to undergo morphological ultrasound study. Mesocardia with an associated LSVC was observed. On careful anatomic examination, no other anomalies were noted. As in the previous case, the heart had an unusual morphology, showing a more rounded shape than normal. There were no additional findings on fetal follow-up, except for intrauterine growth retardation. At 41+2 weeks, a boy was born by forceps delivery, weighing 2450g and with good clinical status. At the time of writing, he is 22 months old and has experienced an episode of acute bronchiolitis and several bouts of severe laryngitis requiring hospitalization.
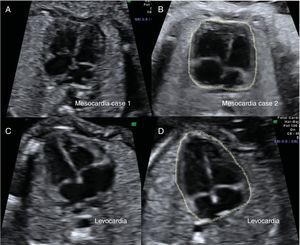
In both these mesocardia cases, the heart showed an atypical morphology (figure 1). On postnatal echocardiography, there were no increases in cardiac trabeculation or myocardial changes in either infant.
 and 2 fetuses with levocardia (C and D). In the fetuses with mesocardia (A and B), the heart is positioned at the center of the thorax and the interventricular septum is aligned with the thoracic midline. In both cases, the hearts have a squared-off shape that contrasts with the triangular shape of the hearts in levocardia (C and D).")
Comparison of heart morphology. Transverse view in 2 fetuses with mesocardia (A and B) and 2 fetuses with levocardia (C and D). In the fetuses with mesocardia (A and B), the heart is positioned at the center of the thorax and the interventricular septum is aligned with the thoracic midline. In both cases, the hearts have a squared-off shape that contrasts with the triangular shape of the hearts in levocardia (C and D).
Within the fetal thorax, a normal position of the heart and orientation of the interventricular septum with the midline are constant features. Variations in this pattern suggest the presence of a diaphragmatic, cardiac, or pulmonary anomaly. Assessment of the cardiac position in the fetal thorax is an important component of 4-chamber examination during routine imaging.2
Comparison of the morphology of hearts in mesocardia with those in levocardia shows a more rounded left ventricle than normal, without the typical inverted cone shape. The tip of the heart does not have the usual apical form, resulting in a morphology different from that of a heart in levocardia.
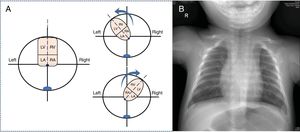
In 1971, Lev et al.3 described the anatomic characteristics of midline hearts. These authors performed autopsy study of 13 cases and reported that the abnormal morphology has an embryologic origin. In normal conditions, after the heart has completely formed and reached a size of 20 to 25mm, there is no true apex and it has a shape similar to that of a heart in mesocardia. In the following phase, the heart points toward the left or right and attains an apical shape (figure 2A). Lev et al. reported that the apex may be hidden or “absent” in midline hearts. In the area where the apex should be, there is a wide stretch of ventrally oriented muscle fibers. It is this distribution that confers the tear shape seen on chest radiology studies (figure 2B).

Morphology of the midline heart. A, diagram of the final phase of fetal embryology, when the cardiac axis changes and the heart acquires its final form. B, anteroposterior chest radiograph of the second case depicts the heart in the center of the thorax with a teardrop- or dewdrop-shaped silhouette. RA, right atrium; LA, left atrium; RV, right ventricle; LV, left ventricle.
Allan et al.4 reported that the cardiac apex points in an anterior direction at 9 weeks and rotates toward the fetal left at 11 weeks. McBrien et al.5 evaluated the cardiac axis in 188 fetuses between 8 and 15 weeks of gestation and also concluded that the fetal cardiac axis has a midline position at 8 weeks’ gestation and undergoes levorotation at the end of the first trimester. The normal, levorotated position is attained at approximately 12 weeks.
The looping that occurs in the fetal cardiac axis at the end of the first trimester is one of the last phases of cardiac embryogenesis. During normal looping, a complex series of changes takes place in the position of the heart.6 At the beginning of this process, the ventricles have a craniocaudal relationship. In the final phase, the heart rotates in a counterclockwise direction around the basal-apical axis, with the right ventricle moving ventrally. This final phase and the relatively late changes occurring in the shape of the left ventricle can explain the change in the cardiac axis seen in early fetal echocardiography.5 Thus, midline hearts that do not complete this final embryological phase show both a change in the cardiac axis and an abnormal apical morphology.
An associated persistent LSVC was present in both cases described, and 1 fetus showed intrauterine growth retardation. Persistence of the LSVC tends to be more common in hearts in mesocardia than those in levocardia associated with congenital heart disease.3 Of the 13 cases described by Lev et al., 6 (46%) were associated with this vascular anomaly. Development of the innominate vein and LSVC involution occur at the end of cardiac morphogenesis, at the same time as looping of the cardiac axis.
Detection of primary mesocardia in the second trimester of gestation in a structurally normal heart is quite unusual. In most cases, mesocardia is associated with major cardiac or extracardiac defects; hence, meticulous study of the fetal anatomy should be performed. The 2 cases diagnosed in our unit showed the atypical morphology described by pathologists. A familiarity with the characteristics of these hearts facilitates prenatal treatment and parental counseling about this condition, and may avoid overdiagnosis of other cardiac conditions.