Invasive management in frail patients with non–ST-segment elevation myocardial infarction (NSTEMI) remains controversial. We investigated the impact of various geriatric conditions.
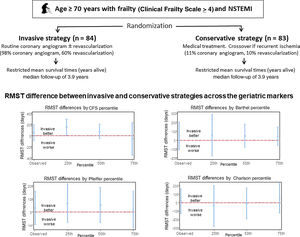
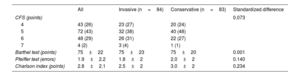
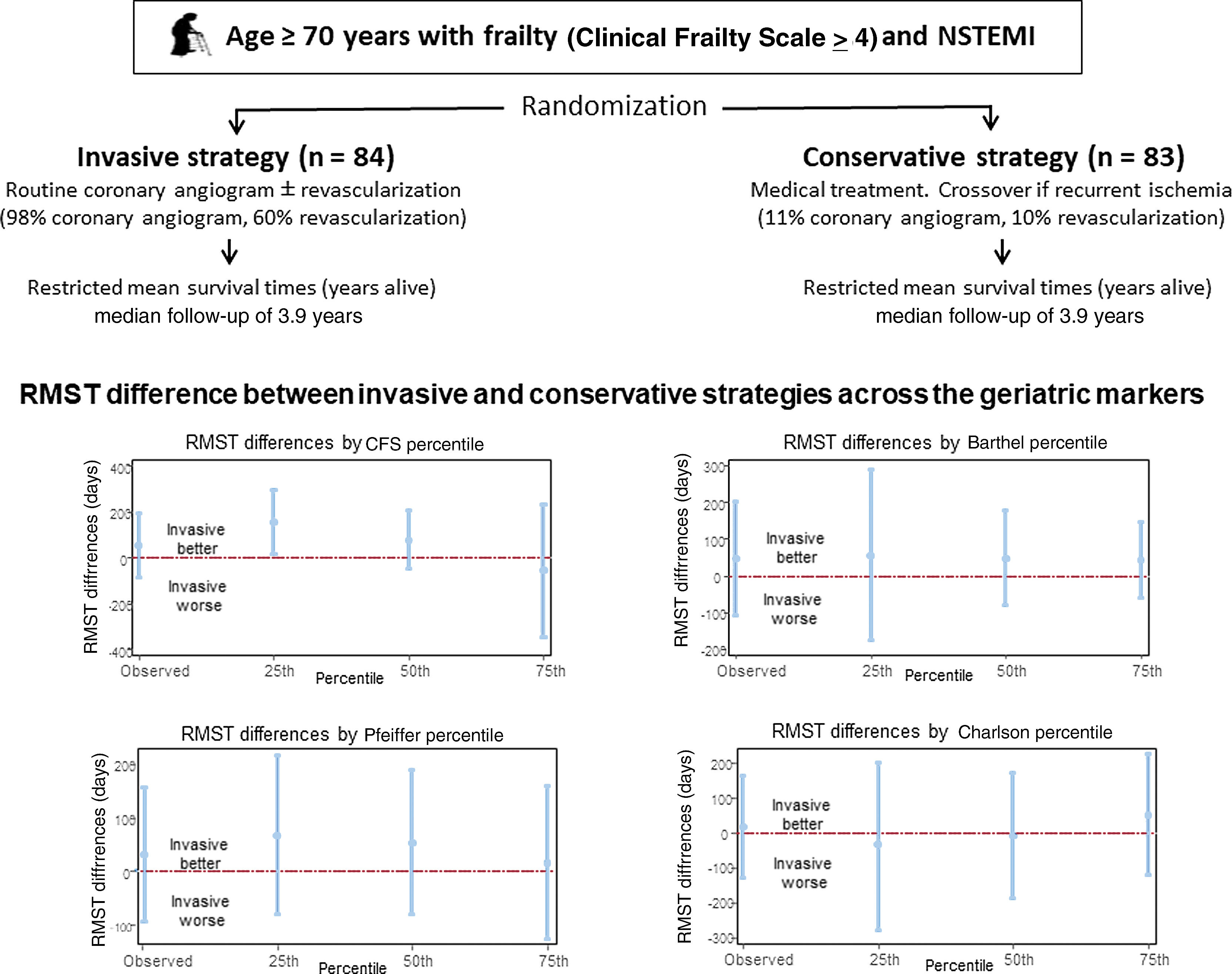
MethodsThe MOSCA-FRAIL trial included 167 adults aged ≥ 70 years with frailty (Clinical Frailty Scale [CFS] ≥ 4 points) and NSTEMI, who were randomized to either an invasive (n=84) or conservative (n=83) strategy. In addition to frailty, we measured activities of daily living (Barthel index), cognitive impairment (Pfeiffer test), and comorbidities (Charlson index). The primary endpoint was the difference (invasive minus conservative) in restricted mean survival time (RMST) for all-cause mortality at a median follow-up of 3.9 years.
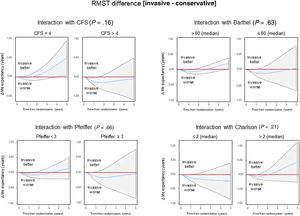
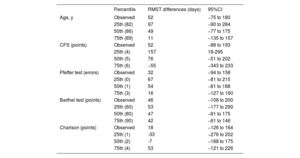
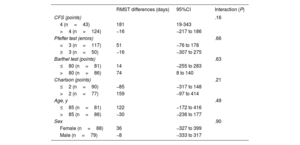
ResultsA total of 93 patients died. The RMST difference favored invasive management at the CFS 25th percentile (CFS=4; 157 days, 95%CI, 18-295; P=.027), which changed to a nonsignificant effect at the 50th and 75th percentiles. The RMST difference remained nonsignificant, irrespective of the severity of other geriatric assessments. In time-to-event analysis, invasive management was associated with an initially lower life expectancy, peaking at around 1 year, among all subgroups. However, patients with CFS=4 experienced a benefit at the end of follow-up (181 days, 95%CI, 19-343), whereas those with CFS >4 did not (−16 days, 95%CI, −217 to 186; interaction P=.16). Subgroups defined by other geriatric markers showed a similar time-dependent trend, albeit with weaker statistical interaction.
ConclusionsAmong adults with frailty and NSTEMI, the CFS might be useful for evaluating the relative risks and benefits of invasive management. A CFS >4 could serve as a valuable threshold for decision-making.
Keywords
Identify yourself
Not yet a subscriber to the journal?
")
Purchase access to the article
By purchasing the article, the PDF of the same can be downloaded
Price: 19,34 €
Phone for incidents
Monday to Friday from 9am to 6pm (GMT+1) except for the months of July and August, which will be from 9am to 3pm