

The European Society of Cardiology (ESC) and the European Respiratory Society (ERS) have recently published new guidelines for the diagnosis and treatment of pulmonary hypertension (PH),1 replacing the 2015 ESC/ERS Guidelines2 and updating the hemodynamic definition proposed by PH experts at the 6th World Symposium of Pulmonary Hypertension held in Nice in 2018.3
For hemodynamic diagnosis, the pulmonary vascular resistance (PVR) cutoff level has been lowered from 3 to 2WU, thus redefining pulmonary arterial hypertension (PAH) as mean pulmonary arterial pressure (mPAP)> 20mmHg with pulmonary arterial wedge pressure (PAWP) <15mmHg and PVR above 2WU. Group2 postcapillary PH is redefined as mPAP> 20mmHg, PAWP> 15mmHg, and PVR <2WU, and combined precapillary and postcapillary PH is redefined as mPAP> 20mmHg, PAWP> 15mmHg, and PVR> 2WU. The new hemodynamic definition is based on population studies confirming the normal range for mPAP and PVR.
The impact of changes to the hemodynamic criteria of the earlier consensus guidelines has been specifically studied in patients with systemic sclerosis (SSc).4,5
The aim of our study was to determine the impact of the new grading criteria on patients who underwent right heart catheterization (RHC) at our hospital between September 1, 2019 and July 31, 2022 and who had an indication for a PH study due to unexplained dyspnea or for PAH screening in the case of SSc.
A total of 74 RHCs were performed as per the protocol in our hospital, and all patients gave written informed consent. According to the previous guidelines, 40 (54%) patients did not meet the criteria for PH whereas 8 (10.8%) were classified as group1, 22 (29.7%) as group2, and 4 (5.4%) as group4; all of these patients retained the PH diagnosis on application of the new criteria.
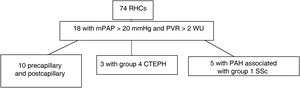
The new definition impacted 18 (24.3%) patients with mPAP> 20mmHg and PVR between 2 and 3WU. Among these patients, 10 with postcapillary PH were reclassified as combined precapillary and postcapillary PH, 3 patients with chronic thromboembolic disease were reclassified as having chronic thromboembolic PH (group 4), and 5 patients with SSc met the criteria for PAH (group1) (figure 1).

Table 1 lists the hemodynamic data for the 8patients reclassified as group1 and group4 PH according to the new 2022 grading criteria.1
Hemodynamic parameters of right heart catheterization with PVR between 2 and 3 WU
| Disease | mPAP, mmHg | PAWP, mmHg | PVR, WU |
|---|---|---|---|
| CTED | 28 | 12 | 2.7 |
| CTED | 24 | 14 | 2.8 |
| CTED | 21 | 6 | 2.1 |
| SSc | 29 | 14 | 2.8 |
| SSc | 26 | 13 | 2.9 |
| SSc | 21 | 7 | 2.4 |
| SSc | 34 | 14 | 2.6 |
| SSc | 22 | 11 | 2.1 |
CTED, chronic thromboembolic disease; mPAP, mean pulmonary arterial pressure; PAWP, pulmonary arterial wedge pressure; PVR, pulmonary vascular resistances; SSc, systemic sclerosis; WU, Wood units.
In all, the disease diagnosis was changed for 8 (10.8%) of the 74RHCs performed. The guidelines provide no specific recommendation for starting a specific drug therapy for these patients, but close follow-up is necessary to monitor for signs of progression.
In view of these results, we believe it is necessary to review the RHC results of patients with a suspicion of PH, especially in high-risk subpopulations, such as SSc, chronic thromboembolic disease, or high-risk genetic mutations.
FUNDINGNone.
AUTHORS’ CONTRIBUTIONSJ.L. Callejas Rubio, E. Moreno Escobar, E. Navascues Martinez, P. Martín de la Fuente, T. Gil Jiménez, and N. Ortego Centeno have contributed to the article as follows: a)substantial contributions to the conception and design, data acquisition, analysis, and interpretation; b)manuscript drafting and critical review; c)final approval of the published version, and d)assumption of responsibility for all aspects of the article and for investigating and resolving any issue with the accuracy and veracity of any part of the project.
CONFLICTS OF INTERESTNone declared.