To the Editor:
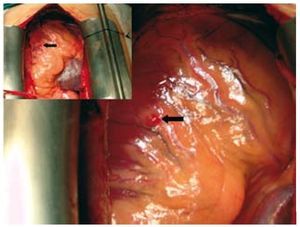
Embolisms from valvular warts form part of the clinical spectrum for presentation of endocarditis. Although in theory they can affect almost any vascular area, presence in the coronary territory is particularly infrequent thanks to the anatomical and haemodynamic properties of the cardiovascular system. We present the case of a 36-year-old man, an ex-intravenous drug addict, HIV positive, hepatitis C positive, with pulmonary hypertension and 2 episodes of mitral endocarditis caused by Enterococcus faecalis 61 months earlier, and mitral and tricuspid endocarditis caused by Staphylococcus aureus 16 months earlier, for which he received the relevant antibiotic treatment with good clinical development. Following an NYHA III cardiology study, severe mitral and tricuspid insufficiencies were found and referred for surgical intervention with double reparative valvuloplasty. The arrow in Figure 1 shows the lesion described below, which corresponds to the intraoperative image taken from the position of the anaesthetist at the patient's head-end (the larger image shows this in detail).

Figure 1. Intraoperative image and detail of the incidentally found lesion; the black arrow shows the interruption of a tributary epicardial coronary branch from the right coronary artery.
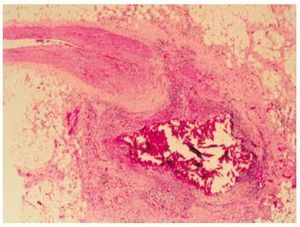
Intraoperatively an epicardial lesion measuring 0.5´0.5 cm was found, with an erythematous surface located on the front free face of the right ventricle, in a tributary region of vascularisation with collateral branches from the right coronary artery, in view of the interruption arising from one of these vessels. Prior to any cannulation procedure or opening of cavities, faced with the superficiality of the lesion and its potentially septic nature despite previous antibiotic treatments, extirpation was decided upon, with the aim of preventing subsequent endocardial contamination during the surgical procedure once the cardiotomy was carried out. Via the use of a haematoxylin-eosin stain, Figure 2 shows a longitudinal section of the wall of a coronary vessel within the context of epicardial fat and minimal remainders of myocardia from the removal bed. The anatomopathological analysis describes the absence of signs of transmural inflammation or intraluminal infiltrate with their three tunics clearly defined and with normal blood cells in their lumen. The normal histology of the vessel is abruptly interrupted by a granulomatous formation, made up of a chronic inflammatory component of lymphocytes and giant mononucleous cells around an interior content of necrosis and ectopic calcification; it is unknown whether the origin of this calcium is the valvular embolus itself or whether it is degenerative on the granulomatous lesion. The diagnosis offered is isolated epicardial granuloma depending on the topography of a coronary vessel with no signs of vasculitis compatible with coronary embolism. Due to the small size of the removed piece, it was not sent for microbiological study so as not to deteriorate its tissue architecture during fractionation. It was therefore preferable to send it all for anatomopathological study, as there were bacterial colony structures that could be seen under microscopic analysis. The significance of this case lies in the fact that it unites the rarity of this complication within the array of signs for septic endocarditis, as already described in existing literature,1-3 with the fact of having presented itself in such a silent way that it was an intraoperative incidental finding. The patient had not had acute coronary syndrome before, very probably due to the reduction of the affected distal vessel. The microscopic image taken from the anatomopathological study of the lesion is also of particular value.

Figure 2. Microscopic image of the haematoxylin-eosin stain of the removed lesion, including a longitudinal section of the branch of right coronary artery amputated due to the abscess following valvular embolisation, all of this within the context of epicardial fat.
Publicly financed by the Provincial Government of Valencia and Regional Ministry of Health of the Community of Valencia.