
To the Editor:
We present the case of a 50-year-old woman whose only signs of cardiovascular risk were smoking and morbid obesity (body mass index = 53). The patient was admitted for vascular surgery due to acute arterial ischaemia in the left lower extremity and obstruction of the external iliac artery was observed. The patient was treated with intra-arterial fibrinolysis, which was efficient initially but early reocclusion followed.
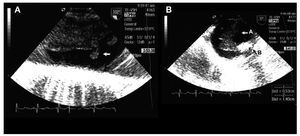
With the aim of localising possible sources of embolism, a transoesophageal echocardiography was carried out which showed a complex aortic atheroma with mobile thrombus at the thoracic aortic level behind the exit of the left subclavian (Figure 1). The thoracic computerised tomography showed an extension of the thrombus to the infradiaphragmatic aorta, reaching close to the coeliac trunk (Figure 2).

Figure 1. A: saggital section of transoesophageal echocardiogram with pendunculated, mobile thrombus in the thoracic aorta. B: 5.3 mm complex plaque (arrow A) with image of ulceration (arrow B) where the thrombus was anchored.

Figure 2. Saggital section of thoracic computerised tomography after contrast with thrombus image at upper descending thoracic aortic level (arrow), with extension to aortic infradiaphragmatic level.
Surgical treatment was offered as the first therapeutic option, which the patient rejected, so oral anticoagulation treatment was initiated. Subsequent development was marked by peripheral recurrent embolisms in the same extremity despite adequate therapeutic INR values. Amputation of the extremity was eventually required.
Thrombi in the thoracic aorta are an uncommon condition associated with atherosclerotic lesions, ulcers, or aortic dilations and they are a potential source of embolisms.
The use of transoesophageal echocardiography provides excellent spatial resolution and allows for the detailed visualisation of the intimal surface.1,2
Treatment of floating thrombi in the aorta is currently a controversial subject and it has only been looked at in retrospective studies.3
There are various therapeutic options, such as anticoagulation,1 thrombolysis, thromboaspiration, balloon catheter thrombectomy,4 open thrombectomy, thromboendarterectomy, or prosthetic aortic replacement.5-7 The exclusion of the thrombus via implantation of an aortic endoprosthesis is under development.
Some authors recommend starting anticoagulation with heparin for 2 weeks, with subsequent reassessment of thrombus development via transoesophageal echocardiogram. If the issue is resolved, chronic oral anti-coagulation is initiated; if it persists, heparin treatment is continued, and surgery is reserved for cases of recurrent embolism.
Other authors (as in the case mentioned, given the physical characteristics of the thrombus and premature reocclusion following arterial fibrinolysis) advocate for a more aggressive treatment once the diagnosis has been made, rather than deterioration at a later stage.
Currently under development is endovascular treatment with thrombus exclusion and coverage of the aortic wall with endoprosthesis, to thereby treat the mobile thrombus and the underlying cause (atheromatous plaque, aortic ulcer, etc).8 In this way recurrences are avoided and subsequent management with anti-aggregation is possible which avoids anti-coagulation.
Despite the lack of randomised tests (given the small number of cases) and in view of the rare complications and good results obtained (in large measure avoiding embolism recurrence), invasive strategies via exclusion of the floating thrombus with the implant of a vascular endoprosthesis has to be considered as an early treatment measure, thrombus location permitting.