Comparative studies of radiofrequency catheter ablation and cryoablation for nodal reentrant tachycardia report similar short-term outcomes, with success rates above 95%.1,2 Of note is the fact that radiofrequency ablation is associated with a risk of atrioventricular block of 0.75%,1 whereas no cases of permanent atrioventricular block have been reported with cryoablation. In contrast, a higher recurrence rate has been reported after cryoablation with 4- and 6-mm catheters, although this problem can be overcome by increasing the lesion size with 8-mm catheters.
Our objective was to assess the efficacy and safety of cryoablation of nodal reentrant tachycardia with an 8-mm catheter immediately after the procedure and after a 1-year follow-up and to analyze the possible factors associated with long-term success.
We retrospectively reviewed our experience of consecutive patients with this type of arrhythmia who were treated with an 8-mm cyroablation catheter (Freezor® MAX, Medtronic; Minneapolis, Minnesota, United States) between May 2008 and January 2013 and who were in clinical follow-up for at least 1 year.
The cyroapplications were performed at –80°C, preferably at the lower third of the Koch triangle, with the aim of abolishing or modifying conduction in the slow pathway and suppressing the inducibility of tachycardia. During these ablations, the patients underwent electrophysiological assessment, and application was interrupted in the event of lack of efficacy.
At the beginning of the study period, the duration of cryoapplications after initial success was 4minutes (23 patients), whereas in the last 18 months, the duration was 8minutes (39 patients). Neither freeze-thaw-freeze cycles nor safety applications were used.
After the procedure, all antiarrhythmic drugs were discontinued and the patients entered clinical and electrocardiographic follow-up for 12 months or until clinical recurrence. Recurrence was defined as persistence of symptoms with electrocardiographic documentation of the arrhythmia.
The demographic characteristics of the patients and the main findings are summarized in Table. An initial successful outcome was achieved in 61 of the 62 patients (98%). In 8 patients (12.9%), transient atrioventricular block was documented during the cryoapplications (PR prolongation). In all patients, this event completely resolved within seconds of interrupting the application. There were no other complications.
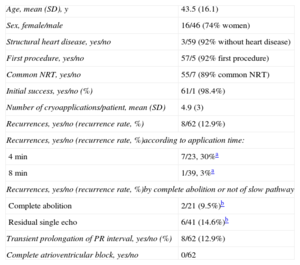
Clinical Characteristics of the Patients and Outcomes
| Age, mean (SD), y | 43.5 (16.1) |
| Sex, female/male | 16/46 (74% women) |
| Structural heart disease, yes/no | 3/59 (92% without heart disease) |
| First procedure, yes/no | 57/5 (92% first procedure) |
| Common NRT, yes/no | 55/7 (89% common NRT) |
| Initial success, yes/no (%) | 61/1 (98.4%) |
| Number of cryoapplications/patient, mean (SD) | 4.9 (3) |
| Recurrences, yes/no (recurrence rate, %) | 8/62 (12.9%) |
| Recurrences, yes/no (recurrence rate, %)according to application time: | |
| 4min | 7/23, 30%a |
| 8min | 1/39, 3%a |
| Recurrences, yes/no (recurrence rate, %)by complete abolition or not of slow pathway | |
| Complete abolition | 2/21 (9.5%)b |
| Residual single echo | 6/41 (14.6%)b |
| Transient prolongation of PR interval, yes/no (%) | 8/62 (12.9%) |
| Complete atrioventricular block, yes/no | 0/62 |
NRT, nodal reentrant tachycardia; SD, standard deviation.
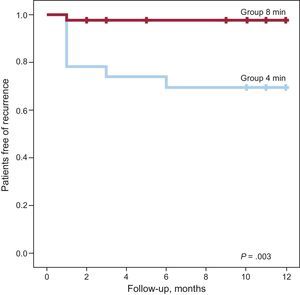
After a mean follow-up of 10.7 months (95% CI, 9.8-11.5 months), 8 patients (12.9%) with successful initial outcomes experienced recurrence, in all cases within 6 months of cryoablation (Figure).

Significant differences were found in the recurrence rate in patients who received 4-minute cryoapplications (7 of 23, 30%) vs those who received 8-minute cryoapplications (1 of 39, 3%; P=.003).
There were no significant differences in the recurrence rate according to the initial outcome of cryoablation when the the 21 patients with complete abolition of conduction through the slow pathway (recurrence rate of 9.5%) were compared with the 41 patients with residual conduction through the slow pathway with a single echo beat (recurrence rate of 14.6%, P=.4). The other variables analyzed were not associated with a higher recurrence rate.
The main findings in this series of patients with nodal reentrant tachycardia treated with cryoablation with an 8-mm catheter are as follows: a) we confirmed that the initial efficacy in an adult population is very high, with similar success rates to those obtained with radiofrequency ablation; b) the safety profile was excellent, even with 8-mm catheters, which do not allow cryomapping; c) our results suggest that the recurrence rate during the first year can be reduced by extending the duration of initially successful application to 8minutes; d) modification of the slow pathway was not found to be important, as failure to detect anterograde conduction was not associated with better clinical outcome than residual conduction inducing a single echo beat.
The most controversial aspect of cryoablation is the higher recurrence rate associated with this technique compared with radiofrequency (10% vs 4%, respectively).1 There is a lack of comparative studies, but the recurrence rates in the published series with 8-mm catheters of around 5% are lower than those reported with cryoablation with 4- and 6-mm catheters and are similar to those reported with radiofrequency ablation. These results may have been influenced by the conditions in which cryoablation was applied. For example, Chan et al,3 who reported a relapse rate of 5.6%, performed a security freeze in the same area as the successful application, and Peyrol et al,4 who reported a recurrence rate of 4.9%, also mention that they performed an additional application of 4minutes at the site of successful application. Bearing in mind that tissue adherence is lost during periods of heating and thus precision may be lost, we decided to simply extend the duration of cryoapplications from 4minutes to 8minutes in our patients.
If low recurrence rates were to be confirmed in larger prospective series when applications are extended to 8minutes, this catheter and application method could improve the outcomes of treatment of nodal reentrant tachycardia with cryoablation.