

Postcardiotomy cardiogenic shock (PCS) has an incidence between 0.5% and 1.5%, depending on the series, and a mortality over 60%.1,2 Treatment is based on the use of first-line inotropic drugs and vasoconstrictors, followed by short-term mechanical circulatory support devices in refractory cases. In these cases, venoarterial extracorporeal membrane oxygenation (VA-ECMO) is the type of mechanical circulatory support most commonly used.1–3 VA-ECMO provides temporary hemodynamic support, thus promoting myocardial recovery and treatment of the underlying heart disease.2 However, numerous aspects and strategies for the treatment of PCS are still under debate. Most current recommendations are based on expert opinions, given the lack of solid scientific evidence.4 One of the most controversial topics is the cannulation access site.1–5 The most common approaches used for central VA-ECMO are cannulation of the right atrium and ascending aorta, whereas peripheral access generally uses the femoral vein and artery.2,3 There is less experience with several other modalities, for instance, the use of the axillary, subclavian, or innominate artery, as well as cannulation with Dacron grafts.3
Other aspects influencing the clinical progress of these patients are the best settings and optimal time to start mechanical circulatory support, the need for left ventricle (LV) unloading, the measures taken to prevent bleeding and thrombosis, and the weaning strategies. The lack of randomized clinical trials on these and other approaches makes it hard to conclude which measures offer the greatest benefit for these patients.1–6 In addition, the lack of evidence on PCS management results in considerable variability between hospitals, which means that patient treatment is heterogeneous.
In view of the above, the aim of this study was to analyze the current status of PCS management in Spanish hospitals with cardiac surgery departments. For this purpose, an online survey was designed and sent to all of these departments through the Spanish Society of Cardiovascular and Endovascular Surgery.
Among the 50 hospitals with a cardiac surgery unit in Spain, 42 (84%) answered the survey (table 1), 37 (88%) of which are part of the public network. More than 90% of these hospitals have more than 500 hospital beds. Only 2 (5%) hospitals perform >700 cardiac surgeries with extracorporeal circulation, 14 (33%) perform between 501 and 700, 19 (45%) perform between 300 and 500, and 7 (17%) perform <300 surgeries. All hospitals have a primary angioplasty program. Approximately 2 out of 3 (62%) implant long-term ventricular assist devices, and 1 out of 3 (38%) also has a heart transplant program. A total of 33 (79%) of these 42 hospitals have a multidisciplinary unit that care for patients in cardiogenic shock and provide cardiac surgery, advanced heart failure management, interventional cardiology, and critical care. Nevertheless, only 26 (62%) of the hospitals have a protocol for the management of PCS.
Hospitals with cardiac surgery departments participating in the survey, according to autonomous community
| Andalusia | Hospital Universitario Virgen de la VictoriaHospital Regional Universitario de MálagaHospital Universitario Virgen del RocíoHospital Universitario Virgen MacarenaHospital Universitario Virgen de las NievesHospital Universitario Reina SofíaHospital Universitario Puerta del Mar |
| Aragon | Hospital Universitario Miguel Servet |
| Canary Islands | Hospital Universitario de Gran Canaria Doctor NegrínHospital Universitario de CanariasHospital Universitario Hospiten Rambla |
| Cantabria | Hospital Universitario Marqués de Valdecilla |
| Castilla-La Mancha | Hospital General Universitario de Toledo |
| Castilla y León | Hospital Universitario de LeónHospital Clínico Universitario de Valladolid |
| Catalonia | Hospital Universitario Valle de HebrónHospital Clínico de BarcelonaHospital Universitario Germans Trias i PujolHospital de la Santa Creu i Sant PauHospital Universitario de Bellvitge |
| Community of Madrid | Hospital Universitario Puerta de Hierro MajadahondaHospital Universitario Fundación Jiménez DíazHospital Universitario 12 de OctubreHospital Clínico San CarlosHospital Universitario de La PrincesaHospital Universitario Ramón y Cajal |
| Chartered Community of Navarre | Hospital Universitario de NavarraClínica Universidad de Navarra |
| Valencian Community | Hospital Universitario y Politécnico La FeHospital Clínico Universitario de ValenciaHospital General Universitario de ValenciaHospital Universitario del VinalopóHospital General Universitario Dr. Balmis |
| Extremadura | Hospital Universitario de Badajoz |
| Galicia | Hospital Universitario de A CoruñaHospital Álvaro Cunqueiro |
| Balearic Islands | Hospital Universitario Son Espases |
| Basque Country | Hospital Universitario de CrucesHospital Universitario Basurto |
| Principality of Asturias | Hospital Universitario Central de Asturias |
| Region of Murcia | Hospital Clínico Universitario Virgen de la Arrixaca |
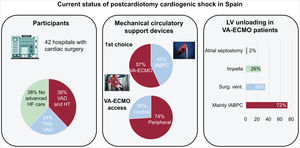
Almost all hospitals (41/42) provide intra-aortic balloon pump contrapulsation (IABPC) and VA-ECMO, 36 (86%) have Levitronix CentriMag temporary ventricular assist devices (Levitronix LLC, United States), and 31 (74%) have Impella transvalvular pumps (Abiomed Inc, United States). The device of choice for the management of PCS is VA-ECMO in 55% of hospitals versus IABPC in 43%. In 3 out of 4 hospitals, peripheral cannulation for VA-ECMO is preferred over central (74% vs 26%) (figure 1). In peripheral accesses, 30 (71%) are performed using an open approach and 12 (29%) percutaneously.

Relevant findings from the survey on postcardiotomy cardiogenic shock management in Spain. HF, heart failure; HT, heart transplant; IABPC counterpulsation, intra-aortic balloon pump counterpulsation; LV, left ventricle; Surg., surgical; VA-ECMO, venoarterial extracorporeal membrane oxygenation; VAD, long-term ventricular assist device; Vent., ventilation.
Only 2 hospitals routinely use LV unloading, whereas 39 (93%) use this strategy according to patient progress (1 hospital reported it does not perform LV unloading). Most often, this technique is performed with IABPC (72%). In addition, 33% also use aspiration cannulas for left chamber unloading as an alternative, 26% use Impella, and 1 hospital uses interatrial septostomy.
These survey results report on the current status of PCS management in Spain (figure 1). Most notably, hospital participation in the survey was very high, indicating the level of interest and concern in the topic. As hypothesized, there is considerable heterogeneity in the approach used with these patients due to the lack of solid evidence to support any particular strategy. Around 1 of every 5 hospitals have no multidisciplinary team to care for these patients, and more than a third have no management protocols. Technical aspects, such as the device of choice, the preferential site for cannulation, the approach of peripheral cannulation or LV unloading, reveal the differences between hospitals. Because this is an extremely urgent condition with a small patient population and high mortality, we believe that randomized multicenter studies should be designed to answer these and other questions. In this regard, Spain has a large and well-formed network of hospitals performing cardiac surgery that could spearhead the resolution of some of these questions through teamwork and collaboration in multicenter studies. The limitations of this study are those related to the survey format. Additionally, 8 (16%) of hospitals with cardiac surgery in Spain chose not to answer the voluntary survey.
FUNDINGNone.
ETHICAL CONSIDERATIONSThis project did not require approval from the Ethics Committee because it was an anonymous survey of Spanish hospitals with cardiac surgery departments. All patients who underwent procedures signed the respective informed consent forms. Possible sex and gender biases have been taken into account in the preparation of this article.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCENo artificial intelligence tool was used.
AUTHOR'S CONTRIBUTIONSJ.E. de Villarreal-Soto wrote the manuscript, prepared the survey, and was responsible for image processing and editing. F.J. Hernández Pérez helped to write and evaluate the survey and reviewed the manuscript. J. García Suárez, J. Rodríguez-Roda Stuart, and S.J. Cánovas López reviewed the manuscript. A. Forteza Gil evaluated the survey and reviewed the manuscript.
CONFLICTS OF INTERESTNone.