Papillary fibroelastomas are the second most common cardiac tumor. These tumors are benign and typically occur in the valvular endocardium, and most present as solitary masses. Only a small percentage cause symptoms. Recurrence of these tumors is exceptional–until now it has not been described in the literature–and the treatment for such cases is unclear.
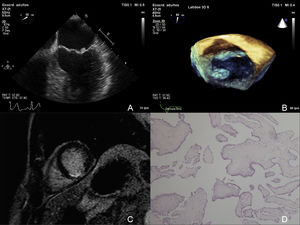
We present the case of a 32-year-old man who presented with a stroke. Transthoracic echocardiography showed a mobile mass attached to the mitral valve causing mild regurgitation, with no other abnormalities. Three-dimensional transesophageal echocardiography (3D-TEE) confirmed the presence of a 6 × 5 mm round tumor, with a friable appearance, attached to the atrial aspect of the mitral valve, at the free edge of the posterior leaflet (P1), suspicious of papillary fibroelastoma (Figure 1). In addition, electrocardiography showed negative T-waves in the inferior leads, and consequently magnetic resonance was performed, which showed a small midsegment-basal subendocardial infarct of the posterior septum and inferior wall (Figure 1).
. C: magnetic resonance showing subendocardial infarct of the posterior septum and inferior wall. D: pathology showing papillary fronds of connective tissue with few cells, covered with a single layer of endothelial cells.")
A and B: 2D/3D transesophageal echocardiogram showing the papillary fibroelastoma on the posterior leaflet (P1). C: magnetic resonance showing subendocardial infarct of the posterior septum and inferior wall. D: pathology showing papillary fronds of connective tissue with few cells, covered with a single layer of endothelial cells.
With this suspected emboligenic papillary fibroelastoma, the patient underwent cardiac surgery, in which the mass was resected, with valvuloplasty using a pericardial patch. The surgical result was good, with no residual regurgitation. Pathology showed papillary fronds of connective tissue with few cells, covered with a single layer of endothelial cells, findings characteristic of a papillary fibroelastoma (Figure 1).
At follow-up, the patient remained asymptomatic, and transthoracic echocardiograms performed every 6 months showed no abnormalities.
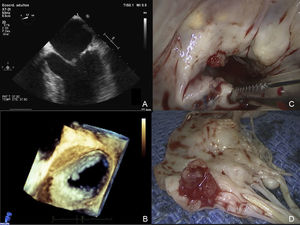
At 2 years postintervention, the patient had sudden-onset low back pain, and renal embolism was diagnosed. Repeat 3D-ETT was performed, which showed a new 4 × 4 mm tumor, with similar characteristics, this time located on the atrial aspect of the anterior leaflet of the mitral valve (A1), just in front of the location of the previous mass (Figure 2).
 C: intraoperative view showing the fibroelastoma and the previous repair of the posterior leaflet. D: gross appearance with multiple papillae resembling a sea anemone.")
Given this rapid tumor recurrence and the aggressive presentation on both occasions (stroke, myocardial infarction, and renal embolism), it was decided to perform mechanical mitral valve replacement (Figure 2). Pathology again confirmed that this was a fibroelastoma.
After myxoma, papillary fibroelastoma is the second most common benign cardiac tumor.1 These tumors originate in the valvular endocardium, mainly in the aortic and mitral valves, although cases have also been described of attachment to the ventricular walls.2 They usually present as solitary masses or, rarely, as multiple lesions.3 They have a characteristic gross appearance, with multiple papillae, resembling a sea anemone. Histologically they are distinguished by a central core of dense connective tissue surrounded by a layer of hyperplastic endocardial cells.
Most patients are asymptomatic and an incidental diagnosis is made on echocardiography, during surgery, or at autopsy.4 A small percentage of patients have severe embolic symptoms, such as myocardial infarction, stroke, or peripheral embolism.5
The initial diagnosis is made by ultrasound. Currently, 3D echocardiography offers better visualization and understanding of the relationship between cardiac structures than 2D imaging, and allows a more precise diagnosis of this type of tumor.
Surgical intervention is recommended for patients who have had an embolic event, or those with large (> 1 cm) or very mobile tumors.1 In asymptomatic individuals with small, less-mobile tumors, the therapeutic approach is debated, but tends to consist of conservative treatment.
In the long-term, the prognosis of these tumors is good, and recurrence after surgical resection has not been described in the literature until now.
We present the first case of recurrent papillary fibroelastoma in the mitral valve. Of note, this recurrence involved very rapid tumor growth, as it was not present on a follow-up echocardiogram performed 5 months previously.
Although a very wide resection of the affected area was performed in the first operation, this was insufficient to prevent the development of a new tumor.
Given that the tumor recurred in the contralateral valve leaflet, right in the area of coaptation of the 2 leaflets, it may be attributed to the continual rubbing that both leaflets are subject to during valve closure, or it may be that we are dealing with a more diffuse involvement of the whole valve.
Although this tumor was histologically benign, its malignant biological behavior with a rapid relapse made it a more aggressive tumor. Therefore, although valve repair would have been technically feasible, we opted for mechanical valve replacement.
.