Acute myocarditis is an inflammatory process of the myocardium. In Spain, the underlying cause is most frequently attributed to viral infection, particularly by Parvovirus B19 and adenovirus.1,2 Many patients are asymptomatic although possible presenting symptoms include arrhythmias, syncope, chest pain, sudden death, heart failure, and cardiogenic shock.
The mortality rate is 20%, and 11% to 50% of patients progress to dilated cardiomyopathy.2
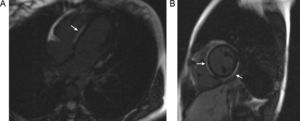
The standard procedure for diagnosis is still endomyocardial biopsy. Magnetic resonance imaging can be very useful as it can detect tissue changes characteristic of the disease, such as edema, hyperemia, necrosis, and fibrosis,3 although experience in pediatric patients is limited.4 Tissue edema is detected as an increase in T2 signal intensity in a focal or diffuse pattern. Hyperemia presents as an increase in early gadolinium enhancement in T1-weighted images, and the irreversible changes due to lesions (necrosis and fibrosis) as an increase in late enhancement. A patchy pattern unrelated to any vascular territory and involvement of the subepicardium with sparing of the subendocardium can provide a differential diagnosis from ischemia (Figure). The presence of 2 of the 3 criteria offers a diagnostic precision of 78%.3,4
 throughout the subepicardium but not in the subendocardium.")
With regard to treatment, support measures and treatment of heart failure are the only interventions shown to improve prognosis.
In our center, a diagnostic protocol is in force in which magnetic resonance and polymerase chain reactions (PCR) analyses to detect viral agents in blood and tracheal aspirate are performed (the latter only in cases of intubated patients). Endomyocardial biopsy is not devoid of risk,5 and we only perform it on patients whose condition is deteriorating. High-dose endovenous gammaglobulins are used for treatment in view of their immunomodulatory and anti-inflammatory effect.
From January 2007 through July 2012, 12 patients were admitted to the intensive care unit diagnosed with acute myocarditis. Diagnosis was established by biopsy (3 patients, 25%) or on the basis of the clinical signs and symptoms with additional tests (echocardiography, electrocardiography, troponin levels, viral PCR) along with a cardiac magnetic resonance scan to confirm the diagnosis. Six of the patients were boys (50%) and 6 girls, with ages ranging from 19 days to 14 years (mean, 3.8 years); 3 patients (25%) were neonates. With regard to the clinical presentation, 10 (83.3%) were in cardiogenic shock requiring inotropic support and 2 (16.6%) had chest pain characteristic of ischemia with ST elevation; 11 patients (91.6%) had substantial systolic dysfunction with a mean [SD] ejection fraction of 32% [10%]. One patient with precordial pain and ST elevation had a normal echocardiography examination (ejection fraction, 60%). Eight patients (66%) required mechanical ventilation and 2 needed circulatory assistance with extracorporeal membrane oxygenation (16.6%).
Magnetic resonance imaging was performed early (in the first 10 days) in 10 patients (83.3%). The most important finding was the presence of a patchy hyperintense pattern in the T2-weighted scan, indicative of edema (9 patients, 90%). Late enhancement was not assessed in the 5 youngest patients (50%) as the myocardial signal could not be eliminated and was positive in 4 of the 5 patients (80%) in whom this assessment could be performed. Early enhancement showed a heterogeneous and patchy pattern.
Viral PCR was done for all patients. The etiologic study was positive in 7 patients (58%); Parvovirus B19 was positive in 4 patients (33% of the sample). In neonates, the virus isolated was enterovirus in 2 patients (16.6% of the sample) and cytomegalovirus in 1 (8.3%). In 3 patients (25%), endomyocardial biopsy was performed and cardiac PCR was positive, with a good correlation with the blood PCR.
Tracheal PCR6 had a low sensitivity, as it was positive in only 1 of the 8 patients (12.5%) in whom this test was done. Troponin T was elevated in all cases and the creatine kinase MB fraction was elevated in 10 (83.3%).
For the mean [SD] follow-up of 398 [155] days, transplant-free survival was 83.3% (10/12). One patient received a transplant 5 months after onset of symptoms, after decompensation, and another patient died in the acute phase during biopsy.
Complete recovery was reported in 8 patients (66.6%) and 2 (16.6%) progressed to dilated cardiomyopathy, with improvement in function compared to the time of diagnosis. With regard to the prognostic factors, the patients who recovered fully had a better ejection fraction and less dilatation on admission, although the difference was not statistically significant, possibly because of the small sample size.
Right ventricular involvement, described as a factor of poor prognosis, was only present in 2 patients (16.6%). Both these were neonates with pulmonary arterial hypertension and their outcome was favorable.
In conclusion, we believe that the most important consideration in acute myocarditis is support measures in the initial phases. Some patients required ventricular assistance, and this was not associated with poor prognosis in the long term. With regard to diagnosis, magnetic resonance imaging is a very useful technique. The main challenge is to obtain high-quality images in younger patients (neonates and infants). Endomyocardial biopsy should only be used in patients with deterioration. With regard to prognosis, right ventricular involvement may be more common in neonates, as they have a marked pulmonary vascular reactivity. In these patients, right-ventricular dysfunction may be secondary to pulmonary hypertension and does not necessarily indicate poor prognosis.