The interrelation between left atrial (LA) morphology and function has not been extensively studied. The type of LA remodelling in response to changes in LA function and the changes in LA function in response to LA remodelling in various cardiovascular diseases could help to elucidate the effects of various therapeutic approaches. Three-dimensional (3D) LA sphericity (LAS) is a comprehensive index of global LA remodelling and has been mainly studied using cardiac magnetic resonance (CMR) and computed tomography in patients with atrial fibrillation (AF). It has been associated with stroke,1 higher CHA2Ds-VASc,2 and success-rates of AF ablation.3 However, assessing 3D-LAS is laborious and requires dedicated software, and access to CMR and computed tomography is lower than that to conventional 2-dimensional (2D) echocardiography. To facilitate LAS assessment, we derived a surrogate metric to estimate 3D-LAS using 2D morphology measurements.
We evaluated patients with paroxysmal or persistent AF who underwent measurement of CMR-based 3D-LAS using dedicated 3D software (ADAS-3D, Spain).4 An experienced imaging cardiologist, who was blinded to the 3D results, manually traced LA endocardial borders and longitudinal and transverse diameters at end-systole in 2-, 3-, and 4-chamber views using conventional 2D-CMR analysis software. Intra- and interobserver variability of the 2D LA morphology parameters was assessed by repeat analyses of 25% randomly selected acquisitions by the initial and a second expert. Informed consent was obtained from all patients at enrolment. The study protocol was approved by the local ethics committee (PI-15-146).
The association between 2D-LAS measurement and 3D-LAS was assessed with linear regression using ordinary least squares, with input variables including patient demographics, all LA measures, biplane LA volume, rhythm during CMR, and left ventricular volumes and mass. Variables with a univariable Pearson r>0.20 were used as input for the multivariable linear regression model. The final model was selected based on an optimal Akaike Information Criterion, with the exclusion of influential outliers (Cook's distance >4) and factors with multicollinearity. Sensitivity analyses were performed to assess slope similarity between AF and sinus rhythm using a linear mixed-effects model with rhythm during CMR as a random effect. The concordance of the models was tested with Lin's concordance correlation coefficient (CCC) and Bland-Altman tests. Variability analyses included correlation coefficients and Bland-Altman tests. Results are presented as mean±standard deviation or median [interquartile range]. All statistical analyses were performed using RStudio (v2023.03; R4.2.1).
We included a total of 80 patients (mean age 59±12 years, 71% male). During CMR, 26% of the patients were in AF. Left ventricular ejection fraction was 62 (55-70)% and 3D-LAS was 82.0±2.9%.
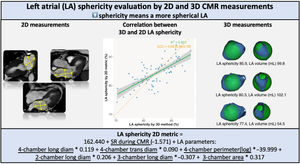
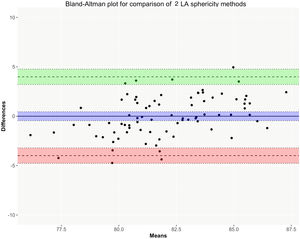
On univariable analyses, the 2D LA measures that were most strongly associated with higher 3D-LAS included 3-chamber area, anteroposterior diameter, and longitudinal to anteroposterior diameter ratio (r=0.35, 0.39 and –0.34, respectively), 4-chamber area and longitudinal diameter (r=0.33 and 0.31), and 2-chamber longitudinal diameter (r=0.31), all P≤.004. The final multivariable linear model to estimate 3D-LAS using 2D LA measurements resulted in r=0.72 and CCC 0.69 and included 4-chamber longitudinal and transverse diameters and perimeter, 2-chamber longitudinal diameter, and 3-chamber longitudinal diameter and area (figure 1). Bland-Altman bias between the 3D measurements and the 2D metric was 0 (limits of agreement –3.99 to 3.99) (figure 2). The model was confirmed by linear mixed-effect regression analyses (r=0.68 and CCC 0.62) with small relative beta differences compared with the metric from –3.45% to 0.83%.

A 2D metric to estimate 3D-LAS was created using linear regression analysis. Diameters and perimeters are measured in mm and area in cm2. 2D, 2-dimensional; CMR, cardiac magnetic resonance; LA, left atrium; Log, logarithmic transformation; Long diam, longitudinal diameter; SR, sinus rhythm; Trans diam, transverse diameter.
 between 3D measurements and the 2D method (Y-axis) to assess LA sphericity. The plot displays the mean difference with 95% confidence interval (95%CI) (blue zone), and similarly the upper and lower limit of agreement defined as the mean difference ±1.96 standard deviation (respectively green and red zone). 2D, 2-dimensional; 3D, 3-dimensional.")
Bland-Altman plot showing the differences (measurement bias) between 3D measurements and the 2D method (Y-axis) to assess LA sphericity. The plot displays the mean difference with 95% confidence interval (95%CI) (blue zone), and similarly the upper and lower limit of agreement defined as the mean difference ±1.96 standard deviation (respectively green and red zone). 2D, 2-dimensional; 3D, 3-dimensional.
Agreements between the 2D LA measurements of the model were good to excellent (all r >0.90, 4-chamber longitudinal diameter r=0.85). Low intra- and interobserver biases were found, such as interobserver diameters biases all<0.92mm.
We report a new and straightforward metric to evaluate LA sphericity based on CMR using 2D LA morphology measurements from standard cine views.5 The metric was coherent in multiple linear regression models, had moderate concordance with 3D-LAS with a fair inter-measurement bias, and the required 2D LA measures had good to excellent intra- and interobserver agreements.
Research on LA function, size and morphology has increased since demonstration of their association with clinically relevant events. However, analyzing atrial function, size, and morphology parameters requires dedicated software and time, especially for atrial morphology. Developing simple and easy-to-apply methods is essential to ensure their implementation in clinical practice. Nonetheless, previous simplified methods for LA morphology assessment may not fully capture complex geometrical remodelling and had limited clinical implications.6 Here we propose a simpler model for 3D-LAS calculation, which comprehensively approximates the complex LA geometry by simple 2D measurements and could help to simplify geometrical LA analysis in future research.
With increasing recognition of the role of atrial dysfunction in different cardiovascular diseases, combined 3D LA morphologic and functional assessments remain promising to quickly obtain more detailed information on atrial remodelling. However, until robust artificial intelligence-based automated atrial assessments provide us with novel and applicable insights, the use of simple 2D measurements has a role to play in assisting us in a comprehensive assessment of LA 3D morphology.
The study population size and phenotype, containing only patients with AF, limit the current findings. Rhythm during CMR was included in the models to account for momentary changes in atrial morphology. The absence of external validation warrants follow-up studies on 2D and 3D LA sphericity. Finally, the addition of other unexplored factors could enhance the concordance with 3D-LAS and reduce the measurement bias.
FUNDINGNot applicable.
AUTHORS’ CONTRIBUTIONSAll authors have participated in the work and have reviewed and agree with the content of the article.
CONFLICTS OF INTERESTV. Delgado has received speaker fees from Abbott Vascular, Edwards Lifesciences, GE Healthcare, Medtronic, Merck Sharp & Dohme, and Novartis. A. Bayés-Genís has received honoraria for lectures and/or advisory boards from Abbott, AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, Roche Diagnostics and Vifor. F. Bisbal has received consulting and speaker fees from Abbot, Biosense Webster and Biotronik. The remaining authors have no conflicts of interest to declare.