

To determine the incidence of sports-related sudden cardiac death in Spain, and to identify the clinical-pathological characteristics, substance abuse, and sports activity associated with this entity.
MethodsRetrospective, population-based, multicenter study of forensic autopsies conducted in 25 provinces during an 8-year period (2010-2017).
ResultsWe investigated 288 cases (98.6% occurred in men with a mean age of 43.8±14.4 years). The incidence in the general population was 0.38 cases out of 100 000 inhabitants per year (0.82 among regular athletes), and most cases (54%) occurred in persons aged between 35 and 54 years. The most frequent sports (96% recreational) were cycling (28%), football (18%), and jogging (17%). Death was of cardiovascular origin in 99%. The main causes were ischemic heart disease (63%), cardiomyopathies (21%), and sudden arrhythmic death syndrome (6%). In young people, cardiomyopathies (38%) and ischemic heart disease (30%), present after the age of 20 years, were the most prevalent. The disease was diagnosed during life in 23 cases, relevant clinical antecedents were observed in 30 cases, and cardiovascular risk factors, mainly obesity, in 95 cases. Toxicological analysis detected cardiotoxic substances in 7%, highlighting the association between cannabis and acute ischemic heart disease.
ConclusionsSports-related sudden cardiac death in Spain has a very low incidence and affects middle-aged men practicing recreational sports, mainly cycling, football, and jogging. This entity is of cardiovascular origin with early onset of ischemic heart disease. Clinical data and substance abuse should be taken into account to develop preventive strategies.
Keywords
Sports activities have clear benefits for cardiovascular health. Sports-related sudden death (SRSD) is an infrequent but catastrophic event with relevant clinical and social implications.1–16
Athletes should be screened for potentially fatal silent heart disease before participating in sporting activities.1 The prevention of SRSD could be improved by having reliable data available on its incidence, precipitating clinical and toxicological factors, and causes of death through forensic autopsies. An ideal approach to this entity would be the creation of multidisciplinary registries with prospective patient inclusion.1,8,12 In 2010, the Spanish Sports-Related Sudden Death Study was launched with the participation of the Spanish Society of Cardiology, the Spanish Sports Council, and the Spanish Society of Forensic Pathology: however, monitoring was not conducted.17
In recent years, various studies have addressed the issue of SRSD.1–16 We draw special attention to the work of Suárez-Mier et al., which was based on forensic autopsies.2,3 However, these studies do not provide accurate figures and only partial clinical-pathological data are available. Furthermore, studies based on emergency records, death certificates, or the mass media do not show the actual causes of death, and studies with selected samples of competitive or military athletes4,6 or those based on reference centers2,3,7,8 do not show the actual magnitude of the problem in the general population. Other hindrances include the absence of a uniform methodology and homogeneous diagnostic criteria. Finally, there are very few studies on cardiotoxic substances that may trigger SRSD.18,19
This study attempted to determine the incidence of SRSD in a large general population, as well as its clinical characteristics, causes of death, toxicological results, and sporting activities associated with this entity. This approach may provide more accurate information that could be used to develop preventive strategies.
METHODSLegislationA forensic autopsy is required in cases of violent deaths, deaths due to suspected criminal activity, and sudden unexpected deaths. This type of investigation is conducted by the Spanish Forensic Pathology Services (FPS) of the Institute of Forensic Medicine and the Institute of Forensic Sciences, and the Spanish National Institute of Toxicology and Forensic Sciences (INTCF).
Study design. Identification of casesThe study design comprised a retrospective population-based multicenter registry of forensic autopsies of SRSD victims conducted over an 8-year period (2010-2017).
SRSD is defined as an unexpected death that occurs during sporting activities or up to 1 hour later in the absence of trauma or violence.20 Competitive sports include any sporting activities that have been certified by a recognized sports authority or association. We included all cases investigated in the FPSs of Seville and the Basque Country, the family heart disease section of the FPS of Valencia, and the histopathology service of the INTCF of Madrid, which is a reference center for 9 autonomous communities. Autopsies are performed in the FPS of each province, but particular cases can be referred to the INTCF by the forensic pathologist when deemed necessary. The study included 25 provinces with a combined population of 23 011 848 individuals (approximately 50% of the Spanish population) (figure 1).
Autopsy protocol from which the cases were obtained.")
The autopsy protocol includes family and personal antecedents (information obtained from medical antecedents and interviews with family members), circumstances of death, complete autopsy, and toxicological analysis of blood, urine, and vitreous humor.21 In line with international recommendations, macroscopic and histopathological studies were performed by forensic pathologists with experience in cardiovascular pathology.22,23
Variables analyzedWe analyzed demographic variables, the cause of SRSD, family and personal antecedents, cardiovascular risk factors (CVRF), toxicological data, type of sport, and sport modality.
Clinical-pathological criteria were applied to determine the cause of death.2,3,21 The following groups were established: sudden cardiac death (SCD) due to acute ischemic heart disease (coronary atherosclerosis with acute thrombosis or acute myocardial infarction); SCD due to chronic ischemic heart disease (coronary atherosclerosis with stenosis more than 75% of the lumen diameter of at least 1 major coronary artery or infarct scarring); SCD due to myocardial disease; sudden arrhythmic death syndrome (SADS) (SCD in a structurally normal heart with probable channelopathy21); and SCD due to other disease, sudden extracardiac death, or sudden death with inconclusive data.3,21 Mortality was coded as sudden death with inconclusive data when no cause of death was found and the autopsy was incomplete.
Toxicological analysis included drugs of abuse, alcohol (≥ 0.5g/L), psychopharmaceuticals, other drugs, and anabolic steroids.
Statistical and epidemiological analysisContinuous variables are expressed as mean±standard deviation and sometimes as interval. Categorical variables are expressed as frequency and percentage. Percentages were calculated excluding cases with unknown data. The means of the quantitative variable were compared using one-way analysis variance. Categorical variables were compared using the chi-square test. Statistical analysis was performed using the SPSS for Windows version 21.0.
To determine associations between certain sports modalities and a higher risk of SRSD, we compared the number of SRSDs in each sport modality and the number of people practicing that sport in the general population in 2015.24
The SRSD mortality rates were calculated based on the Spanish National Institute of Statistics 2011 population census figures obtained in the 3 provinces with the highest levels of registration (n=4 499 248). Their distribution by sex and age is shown in the additional material (). Data from the INTCF were excluded because it is a reference center. These rates were extrapolated to the Spanish population to calculate the expected annual number of SRSDs. Finally, the expected SRSD mortality rates were calculated for the population that practices sport each week, using as references the 2015 Spanish Yearbook of Sports Statistics24 and the Spanish National Health Survey.25
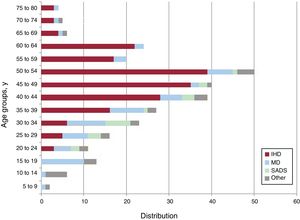
RESULTSGeneral dataDuring the 8-year study period, data were collected on 288 cases of SRSD (98.6% men) (table 1). There was an average of 36 cases per year (29-42). No time trend was observed. Mean age was 43.8±14.4 years. Figure 2 shows the distribution of cases by 5-year age groups. Most cases (54%) occurred in men between 35 and 54 years.
Demographic data, cause of sudden death, clinical antecedents, and toxicological analysis (n=288)
| Service | |
| INTCF | 141 (49) |
| FPS Valencia | 52 (18) |
| FPS Seville | 52 (18) |
| FPS Basque Country | 43 (15) |
| Demographic data | |
| Sex | |
| Men | 284 (98.6) |
| Women | 4 (1.4) |
| Age, ya | 43.8±14.4 (6-80) |
| Cause of sudden death | |
| Ischemic heart disease | 183 (63) |
| Myocardial disease | 60 (21) |
| Sudden arrhythmic death syndrome | 18 (6) |
| Sudden cardiac death due to other causes | 20 (7) |
| Sudden extracardiac death | 4 (1) |
| Inconclusive data | 3 (1) |
| Clinical antecedents | |
| Family antecedents | |
| Yes | 41 (20) |
| No | 164 (80) |
| Unknown | 83 |
| Personal antecedentsb | |
| Cardiovascular disease diagnosed in life | 23 (10) |
| Cardiovascular symptoms in life | 30 (13) |
| Cardiovascular risk factorsc | 95 (42) |
| None | 92 (41) |
| Unknown | 61 |
| Toxicological analysis | |
| Cases analyzed | 263 (91) |
| Positive for cardiotoxic substances | 18 (7) |
| Cannabis | 10 |
| Alcohol (≥ 0.5 g/L) | 4 |
| Drugs that cause QT prolongation | 4 |
| Cocaine | 2 |
| Anabolic steroids | 1 |
| Positive for noncardiotoxic drugs | 24 (9) |
| Negative for noncardiotoxic drugs | 221 (84) |
| Unknown | 25 |
FPS, forensic pathology service; INTCF, Spanish National Institute of Toxicology and Forensic Sciences.
Unknown cases were excluded from the calculation of percentages.
Values are expressed as No. (%) or mean±standard deviation (range).
 by 5-year age group and cause of death. IHD, ischemic heart disease; MD, myocardial disease; SADS, sudden arrhythmic death syndrome.")
SRSDs were of cardiovascular origin in 99% of cases (table 1). The main cause of SRSD was ischemic heart disease (63%: 37% chronic and 26% acute), followed by myocardial disease (21%). The most frequent entities within this category were arrhythmogenic cardiomyopathy (n=18), hypertrophic cardiomyopathy (n=16), idiopathic left ventricular hypertrophy (n=11), and myocarditis (n=6). SADS accounted for 6% of the total number of SRSDs. Other causes were abnormal coronary artery disease (n=5), aortic valve disease (n=5), and thoracic aortic dissection (n=3) (). No statistically significant differences were found between the FPS and the INTCF in the number of cases in the 4 main groups by cause of death.
Mean age was higher in ischemic heart disease (49.1±10.7 years) than in myocardial disease (35.6±15.8) and SADS (34.3±8.4) (P < .001). In people aged 40 years or older, ischemic heart disease was the most prevalent (around 80%). In young people between 20 and 34 years, myocardial disease was the most prevalent (38%), although attention should also be drawn to the percentage of ischemic heart disease (around 30%). Of the 18 cases of SADS, 11 (61%) occurred in this age group. In people 15 to 19 years, myocardial disease was the most prevalent (77%) (figure 2).
Table 1 shows the clinical data. In 41 cases, there were some family antecedents of interest, mainly SCD (n=14), ischemic heart disease (n=13), and arrhythmic syndromes (n=7). In 23 cases, the disease causing SRSD had been diagnosed during life: ischemic heart disease and cardiomyopathy in 9, valvular heart disease in 3, and congenital heart disease and Wolf-Parkinson-White syndrome in 1. Another 30 cases had cardiovascular symptoms, of which the main ones were arrhythmia (n=13), chest pain (n=9), and syncope (n=6). The causes of death were myocardial disease (n=13), ischemic heart disease (n=12), SADS (n=4), and anomalous origin of a coronary artery (n=1). CVRF was recorded in 95 people (42%; 62% more than 54 years): obesity (body mass index [BMI] more than 30 at autopsy) in 45, high blood pressure in 35, dyslipidemia in 32, smoking in 21, and diabetes mellitus in 10. The average BMI was 27.2±4.3.
Toxicological analysis (table 1) was performed in 263/288 cases (91%), showing the presence of substances with cardiovascular effects in 18 cases (7%). Cannabis was detected in 10 cases (together with cocaine, opiates and/or alcohol in 3 of these cases). Acute ischemic heart disease was the cause of death in 8 of these cases.
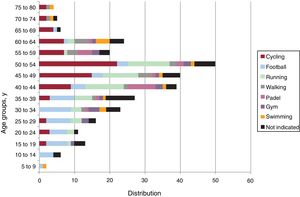
Sporting activityOnly 11 of the deceased (4%, 7 cases aged 30 years or older) practiced competitive sport at the time of death. The most frequent sports were cycling, football, and running (figure 3 and figure 4). Out the 279 cases in which the type of sport was recorded, 156 (56%) practiced outdoor sports and 123 (44%) practiced indoor sports.
 by 5-year age group and sporting activity.")
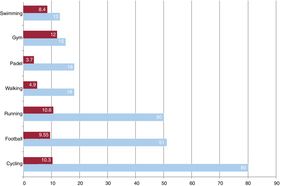
. The red bars represent the percentage of people of the total population analyzed who practice this sport at least once a week. Data obtained from the 2015 Spanish Yearbook of Sports Statistics.24 .")
Comparison of the number of cases of sports-related sudden death cases by sporting activity and the number of people in the general population who practice each sport. The blue bars represent the number of cases of sports-related sudden death in the sample by sporting activity (n=288). The red bars represent the percentage of people of the total population analyzed who practice this sport at least once a week. Data obtained from the 2015 Spanish Yearbook of Sports Statistics.24 .
Figure 3 shows the distribution of sporting activity by age. In persons younger than 35 years, the most frequent sport was football, whereas in those older than 45 years, the most frequent sport was cycling. A high percentage of people between 40 and 54 years practiced running. Due to these variations, the distribution of the causes of SRSD differed between 3 main sports (P=.02). There was a high percentage of ischemic heart disease in those practicing cycling and running, (74% and 60%, respectively) and of ischemic heart disease (43%) and myocardial disease (37%) in those playing football.
CVRFs were more frequent in those who practiced cycling (38%) than in those who practiced running (17%) and football (14%; P=.01). Of note, BMI was higher among those practicing cycling than among those practicing running and football (28.3±4, 26.7±3.2, and 25.1±5.9, respectively; P=.006).
Figure 4 shows the total number of SRSDs in the most frequent sporting activities compared with the frequency of these activities in the general population.24 The highest risk of SCD was in cycling, whereas the lowest risk was in gymnastics and swimming.
Epidemiological dataIn the general population, the incidence of SRSD was 0.38 cases/100 000 population/y (95% confidence interval [95%CI], 0.32-0.48; 0.76 in men vs 0.01 in women). In the population practicing sports each week, its incidence was 0.82 cases/100 000 sportspeople/y (in men, 1.52). According to our projections, the expected annual number of cases of SRSD in Spain would be 167 (165 men and 2 women; 95%CI, 140-211).
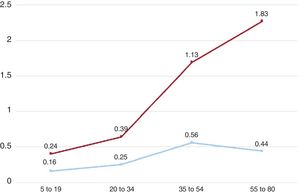
Figure 5 and the supplementary data () show the mortality rates of SRSD by age group. In the general population, the highest incidence was in adults aged between 35 and 54 years. This incidence was double that in those aged between 20 and 34 years and triple that in children and adolescents. In those who practiced sport each week, the incidence progressively increased from the age of 35 years.
 by age group. The red lines represent sports-related sudden deaths in those who practice a sport once a week by age group. Data obtained from the INTCF were excluded from the calculations because it is a reference center.")
Mortality rates for sports-related sudden death by age group in the general population and in those who practice sports once a week. The blue lines represent sudden sport-related death rates in the general population (number of cases/100 000 population/y) by age group. The red lines represent sports-related sudden deaths in those who practice a sport once a week by age group. Data obtained from the INTCF were excluded from the calculations because it is a reference center.
The present study provides relevant epidemiological, pathological, clinical, and toxicological data that could be used to develop prevention and cardiovascular screening strategies in SRSD. Its multicenter design made it possible to obtain one of the largest series of SRSDs and the largest series based on autopsies. This study is the first to investigate such data in a general population of children and adults. Following international recommendations, all cases underwent forensic autopsy.
According to the literature review, there are only 3 epidemiological studies on SRSD in general populations of children and adults. However, in the studies conducted in Germany12 and France,11 the percentage of autopsies was low and therefore the cause of death could only be determined in 45% (66/144) and 25% (203/820) of the cases, respectively. The Australian study10 investigated 147 cases of nontraumatic SRSD, but no clinical or toxicological data were analyzed.
IncidenceMost of the published data have been obtained from series of competitive athletes, suggesting an annual incidence of SRSD of between 1.25/100 000 population/y and 2.5/100 000 population/y.9 However, these figures cannot be extrapolated to the general population. In the present study, the incidence of SRSD was 0.38 cases/100 000 inhabitants/y, which is in line with the average incidence found in the other 3 population studies: Australia, 0.5-0.98,10 France, 0.46,11 and Germany, 0.12.12
The incidence of SRSD is much higher in men than in women, with percentages ranging from 70% to 90%.3,7,10–14 In the present study, its incidence was close to 99%. These percentages may be explained by the higher incidence among men of SCD due to ischemic heart disease and more frequent sporting activities. According to a population survey,25 50% of men and 42% of women practice sport at least once a week. The average time spent on sport per week is higher in men than in women (440.7 vs 269.2min), and more men than women practice cycling (47.1% vs 28.5%), football (35.8% vs 6.3%) and running (33.4 vs 26.7%). However, these results do not completely explain the striking differences between men and women, which may suggest that male sex itself could be a risk factor for SRSD.
Although the medical literature has mainly addressed SRSD in young people, the incidence of SRSD is higher among middle-aged adults.2,3,10–14 We found that the highest incidence was in adults aged between 35 and 54 years. This incidence was double that in those aged between 20 and 34 years and triple that in children and adolescents. These results may be mainly due to the higher incidences of ischemic heart disease and CVRF. In this study, the incidence of SRSD in those less than 36 years was similar to that found in France (0.22) and Denmark (0.19).11,15
Causes of sudden sports-related deathIschemic heart disease is the most common disease in adults (around 70%).10,11,16 Our results are somewhat different from those of Suarez-Mier et al.,2,3 who found a lower percentage of ischemic heart disease.
In line with the results of other studies,2,10,11,15 in our series, cardiomyopathies (38%) were the most prevalent cause in young people, although the percentage of cases with ischemic heart disease was higher than expected (30%). The consumption of certain drugs and foods or exposure to environmental toxins, together with genetic factors, may explain the appearance of early coronary atherosclerosis. A recent study by our group found that the percentage of myocardial disease was significantly higher in persons with SRSD than in those with non-SRSD (44% vs 20%) and that SRSDs were more frequent in persons with arrhythmogenic and hypertrophic cardiomyopathies, followed by myocarditis and dilated cardiomyopathy.19
In our series, the percentage of SADS was less than that in studies conducted in reference centers. This result is probably due to referral bias, which tends to overestimate the number of patients with a more complex diagnosis.
Clinical antecedentsSRSD is usually secondary to silent cardiovascular disease. However, in 10% of cases the disease causing SRSD was known in life, in 13% there were cardiovascular symptoms (mainly palpitations/arrhythmia and syncope), and in 20% there were relevant family antecedents. The frequency of relevant clinical antecedents was particularly high in persons with myocardial disease. These findings may be of relevant to screening programs prior to participation in sporting activities.
In line with the results of the DARIOS population study conducted in Spain,26 we found a high prevalence of CVRFs, mainly obesity, which was common in persons older than 54 years (62%). Overweight is defined as an average BMI of 27.2±4.3 and is more common among persons who practice cycling. Cycling is a sport in which the average age of the participants is higher than that of participants in other sports.
ToxicologyToxicological analysis detected cardiotoxic substances in 7%, mainly cannabis and to a lesser extent cocaine, which could have acted as precipitating factors for the lethal arrhythmia. Acute ischemic heart disease was the main cause of death in these individuals. This percentage is not surprising given the prevalence of drug use in the Spanish general population aged 15 to 64 years during the period 2013 to 2017 (cannabis, 6.6% to 9.1%; cocaine, 1%; and amphetamines, 0.2%).27 This result should be taken into account in the design of preventive strategies. Cannabis has a low risk of cardiovascular morbidity and mortality in people without underlying disease, although the risk of acute myocardial infarction could be increased by its very recent use.28 Ischemic heart disease is the most common morphological substrate of cocaine-related SCD.29 However, in our series, acute ischemic heart disease was more frequently associated with cannabis than with cocaine. We highlight the single case in which the analysis detected anabolic steroids, which have adverse effects associated with SCD.30
Type of sportThe results show that most of the SRSDs occurred in recreational athletes (96%), a percentage that is similar to those found in studies conducted in France (94%)11 and Spain (98%).3
Sports associated with SCD are different from those in the general population. In Spain and France, the distribution of activities is similar: in descending order these are cycling, football, running, and walking. Comparisons between the number of cases of SRSD and the frequency of practice of each sport in the general population by age (figure 3 and figure 4) show that in people older than 39 years the risk of SRSD is higher in those who practice cycling and running than in those who practice gymnastics and swimming. However, people younger than 35 years who play football are at higher risk of SRSD than those of the same age who practice other sports. These results may be related to the high dynamic component (high oxygen consumption) associated with cycling and football, and the high static component (increased blood pressure) associated with cycling.31 Other factors that may account for increased risk among cyclists are older age (higher prevalence of ischemic heart disease) and obesity.
Implications for preventionThe results of the present study are relevant to the development of screening or prevention measures for SRSD. Information on the incidence and causes of SRSD and its sex and age distribution is essential to optimize prevention strategies and the choice of screening tests prior to participation.
In Spain, around half of all SRSDs occur in middle-aged men who practice recreational sports (mainly cycling) and are due to ischemic heart disease. Cases of SRSDs in young professional athletes are very rare. Specific prevention campaigns should focus on adult men by providing advice on the type and intensity of sports activity in relation to the presence of CVRFs, mainly obesity, as well as certain cardiac diseases or symptoms such as arrhythmia, palpitation, and syncope.
Because more than half of SRSDs occur outside sports venues, in addition to having automatic defibrillators available in these areas, the general population should be trained in basic cardiopulmonary resuscitation maneuvers.
LimitationsThe retrospective design of this study entails a number of limitations. Our results on the incidence of SRSD and projections for the general population should be interpreted with caution. Some information on clinical antecedents, demographic data, and anthropometric measurements could not be collected. Although a distinction was made between competitive and recreational sport, we could not collect data on the practice of high-intensity sport in order to assess its level of relative risk. These limitations are inherent to published studies on SRSD. These limitations are also compounded by referral bias arising from cases being reported to the INTCF: its data were excluded from the epidemiological calculations because their inclusion would have led to the incidence of SRSD being underestimated. However, we believe that the results of this study, which was based on a multicenter approach and a large number of forensic autopsies, will serve to improve our knowledge of the risk factors, causes, and types of sport involved in SRSDs in Spain, thus making it possible to establish strategies to prevent these dramatic deaths.
CONCLUSIONSThe incidence of SRSD in Spain is very low and affects men who engage in recreational sports, mainly cycling, football, and running. It is of cardiovascular origin in 99% of cases (63% due to ischemic heart disease). In some cases, there is a history of cardiovascular disease, CVRF, or substance abuse. Data concerning these issues could help to establish prevention strategies. Epidemiological studies relating to toxic and dietary habits or exposure to environmental toxins, together with the study of genetic factors, are needed to improve our knowledge of the appearance of coronary atherosclerosis at such a young age. We strongly recommend that a mandatory national SRSD registry should be created with the participation of forensic physicians and pathologists, sports physicians, cardiologists, and all other relevant parties.
CONFLICTS OF INTERESTNone declared.
- –
Forensic studies on sports-related sudden death in the general population involve methodological limitations that underestimate its actual incidence and provide only partial information on its clinical-pathological characteristics.
- –
This study is the first to investigate SRSDs in a general population (23 million inhabitants). It applied a homogeneous methodology that followed international guidelines.
Supplementary data associated with this article can be found in the online version available at https://doi.org/10.1016/j.rec.2020.05.044