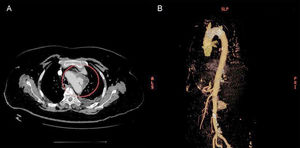
Mycotic aortic pseudoaneurysm is a rare clinical disorder that accounts for a very small proportion of all arterial aneurysms. It is characterized by inflammation of the arterial wall due to the presence of microorganisms. Infective endocarditis, one of the pathogenic mechanisms that leads to vascular infection, is a major cause of arterial pseudoaneurysms. Valvular and ventricular aneurysms also occur but they are less common. The clinical manifestations of infectious aortitis are nonspecific and a high index of clinical suspicion is thus necessary to establish a diagnosis. Early diagnosis and prompt initiation of empirical antibiotic therapy are crucial as pseudoaneurysms are associated with rapid growth and consequently a high risk of aortic rupture and death. We present the case of a 70-year-old Caucasian woman with a pseudoaneurysm due to Salmonella enteritidis treated with endovascular aneurysm repair (EVAR) and targeted antibiotic therapy. The patient had several cardiovascular risk factors (hypertension, dyslipidemia, and diabetes mellitus type 2) and had visited the emergency department 3 times in the space of 4 weeks reporting physical weakness accompanied by considerable asthenia and generalized myalgias. Her past history included chronic ischemic cardiomyopathy. On her last visit to the emergency department, she continued to show signs of general deterioration but in addition had dysphagia, dysphonia, and episodes of choking. She was admitted to hospital and her laboratory workup showed elevated acute phase reactants (C-reactive protein, 304 mg/L; leukocytes, 14 x 103 cells/μL; erythrocyte sedimentation rate, 120 mm/h), accompanied by normocytic and normochromic anemia (hemoglobin, 10.3 g/dL; mean corpuscular hemoglobin concentration, 28.5 pg; mean corpuscular volume, 89 fL). Tumor markers (carcinoembryonic antigen and carbohydrate antigen 19-9) and autoimmune markers (antinuclear antibodies, antinucleoprotein antibodies, and antineutrophil cytoplasmic antibodies) were within normal ranges. A gastroscopy and a computed tomography (CT) scan of the chest, abdomen, and pelvis were ordered to investigate the causes of the dysphagia. The findings of the gastroscopy were unremarkable, but the CT scan showed focal esophageal wall thickening and an aneurysm measuring 16 × 8mm in the aortic arch. One week after admission, the patient experienced episodes of diarrhea and fever (38°C) and we therefore ordered blood cultures and a stool examination. Both the blood and stool cultures grew S enteritidis that was sensitive to several antibiotics. Despite antimicrobial treatment with ciprofloxacin, the fever persisted and the laboratory studies continued to show elevated C-reactive protein (205 mg/L) and erythrocyte sedimentation rate (106 mm/h). Suspecting an endovascular infection, we ordered a second CT scan, which showed progression of the aortic aneurysm (24 × 15 mm) (Figure A). On confirmation of the diagnosis of a pseudoaneurysm due to Salmonella enteritidis and in view of the high comorbidity associated with this condition, the patient was treated with EVAR consisting of the insertion of a Zenith endovascular graft (34 × 77 mm) in the thoracic aorta (Figure B). Following the intervention, the patient was treated with intravenous ceftriaxone and ciprofloxacin for 4 weeks and progressed favorably. Bacteria of the Salmonella genus are the main cause of infectious aortitis and have been implicated in 33% to 50% of all cases.1 Approximately 5% of Salmonella gastroenteritis cases are thought to cause bacteremia, which is complicated by arteritis in approximately 1 in 10 cases.2 Vascular infections due to Salmonella species are much more common in the aorta than in other peripheral arteries, and the thoracic zone is involved in 17% of cases.1 Despite the radical treatment approach, bacterial aortitis is associated with high mortality (up to 36%).3 The most common risk factors are diabetes mellitus and a history of coronary artery disease and hypertension. The signs and symptoms vary according to the site of the mycotic aneurysm and therefore tend to be nonspecific. The most common manifestations, however, are fever, back pain, abdominal pain, and chills. We have included a review of 30 cases of aortitis caused by Salmonella species treated with EVAR since 2003. Of the 30 patients reviewed, 27 (90%) survived and showed no signs of recurrent infection and 3 (10%) died (). There have been recent reports of improved survival rates in patients treated with a combination of EVAR and antibiotics, which can be considered an adequate treatment approach in this setting.4 The optimal duration of antimicrobial treatment following EVAR, however, is still a topic of debate. While some authors recommend treatment for life,4 others have reported resolution after 12 months.5 In conclusion, aortitis due to Salmonella species is rare, but it can be fatal. A better understanding of the clinical manifestations of this condition is necessary to ensure prompt and effective treatment and improved survival outcomes. EVAR could be a particularly interesting option for patients with a high risk of perioperative complications.
ISSN: 1885-5857
Impact factor 2024
4.9
