
Achievement of a maximal workload of 10 metabolic equivalents (METs) is associated with good outcome with events rates of just around 1%/y,1–3 whereas patients with lower exercise capacity have significantly worse outcomes. However, there is little information on common daily exercises that can be quantitatively measured and provide information equivalent to this exercise performance.4 We aimed to assess the ability to climb stairs in patients undergoing exercise testing.
Consecutive ambulatory patients referred for a clinically indicated exercise test were included. After exclusions due to premature interruption of the test for clinical reasons (n = 6) or inability to properly count the stair-climbing exercise time (n=3), we included 165 patients (mean age 66 ±12 years, 55% male) who underwent treadmill exercise testing with an electrocardiogram (n=15) or echocardiography (n=150). All included patients exercised until exhaustion. At least 15minutes after exercise testing, patients were asked to climb 4 flights of stairs (60 stairs) at a fast pace without stopping but also without running. The time to complete the task was recorded. Good exercise capacity was defined as the achievement of 10 METs,1,2 intermediate as the achievement of 8-9.9 METs, and limited exercise capacity as <8 METs.
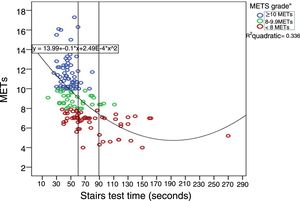
Clinical and exercise testing patient characteristics are listed in table 1. Patients who achieved 10 METs during exercise (n=69) completed the stair-climbing test in 46±11seconds, those who achieved 8-9.9 METs (n=37) in 58±21seconds, and those who achieved <8 METs (n=59) completed it in 82±41seconds (P <.001). The correlation between METs and the stair-climbing test time was 0.53 (figure 1). The area under the ROC curve for the stair-climbing time to predict an achievement of 10 METs was 0.79 (95%CI, 0.72-0.86; P <.001). A cutoff value of 60seconds had high sensitivity (94%) and negative predictive value for 10 METs (93%), although specificity and positive predictive values were 53% and 59%, respectively. A cutoff value of 90seconds had low sensitivity (34%) but high specificity (96%) and positive predictive value (83%) for predicting <8 METs.
Clinical baseline characteristics and exercise results in the 165 patients
| Clinical characteristics | |
| Current smokers | 18 (11) |
| Diabetes | 32 (19) |
| Hypertension | 88 (53) |
| Hypercholesterolemia | 86 (52) |
| History of CAD | 33 (20) |
| Reasons for testing | |
| Chest pain | |
| Typical | 41 (25) |
| Atypical | 40 (24) |
| Noncoronary | 21 (13) |
| Dyspnea | 33 (20) |
| Evaluation of CAD | 9 (6) |
| HCM/valvulopathies | 4 (2) |
| Others | 15 (9) |
| Medications | |
| Beta-blockersa | 14 (9) |
| ACEI/ARA-II | 58 (35) |
| Calcium antagonists | 18 (11) |
| Nitrates | 14 (9) |
| Diuretics | 7 (4) |
| Exercise testing (n=165) | |
| % Achieved of the maximal age-predicted heart rate | 97±16 |
| Symptoms during the test | 31 (19) |
| Positive electrocardiogram | 20 (12) |
| Positive exercise testingb | 44 (27) |
| Exercise echocardiography (n=150) | |
| Resting wall motion abnormalities | 16 (11) |
| Ischemia | 48 (32) |
| Abnormal results | |
| Ischemia +/-resting wall motion abnormalities | 57 (38) |
| Exercise-induced diastolic dysfunction | 3 (2) |
| Noncardiac dyspnea | 2 (1) |
| Exercise-induced abnormalities in HCM/valvulopathiesc | 3 (2) |
| Others | 1 (1) |
| Wall motion score index | |
| Rest | 1.04±0.20 |
| Peak | 1.16±0.30 |
| Left ventricular ejection fraction, % | |
| Rest | 60±6 |
| Peak exercise | 65±11 |
ACEI, angiotensin-converting enzyme inhibitors, ARA-II, angiotensin II receptor antagonist, CAD coronary artery disease; HCM, hypertrophic cardiomyopathy.
Values are expressed as No. (%) or mean±standard deviation.

Abnormal results were seen in 58% of patients with limited exercise capacity, 30% with intermediate exercise capacity, and 29% with good exercise capacity (P=.002), as well as in 32% of patients who completed the stair-climbing test in at least 60seconds compared with 52% of those that took between 61 and 89seconds and 58% of those who took longer (P=.018).
In a previous study measuring O2 consumption in healthy young volunteers, climbing up 70 steps in 1minute equalled 8.6±0.4 METs.5 Most participants able to step up 4 flights of stairs in 1minute in our study performed well during exercise testing. However, the lack of prediction in them is likely because the stair-climbing test consists of a mixture of aerobic and anaerobic evaluation, as it implies achieving a high workload in a short time.
Regardless of this consideration, individuals who cannot complete the stair-climbing test in 1.5minutes are expected to have poor functional capacity and worse exercise test performance and results. In contrast, the range of achieved METs in patients who complete the stairs test in less than 1minute varies more widely. These findings could be of interest for stress testing and stress echocardiography triage strategies.