Keywords
INTRODUCTION
QT interval prolongation is a predisposing factor for the onset of potentially fatal ventricular arrhythmias. It is known to be associated with several drugs, such as antiarrhythmic agents, antibiotics and antihistamines, and has also been related to electrolytic and metabolic alterations.1-3 Methadone is a synthetic opioid that is frequently used to treat heroine addiction and chronic pain. Although there are concerns about its safety, It is generally well tolerated and has few side effects.4 However, it has recently been reported that treatment with high doses of methadone may be associated with ventricular arrhythmia.5,6 We present 4 patients with QT interval prolongation and torsade de pointes (TdP) during methadone maintenance treatment.
CASE STUDIES
Four patients (3 men, 1 woman) with no known history of heart disease were seen in the emergency room for syncopal episodes (Table). All were under long-term methadone therapy, although only 1 was receiving >200 mg/day. Three of these patients were infected with human immunodeficiency virus (HIV), but only 1 was on antiretroviral therapy.

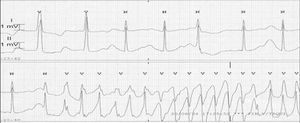
The electrocardiographic recordings and monitoring showed sinus rhythm, prolonged corrected QT interval, and runs of self-limiting TdP polymorphic ventricular tachycardia (Figure 1), which degenerated to ventricular fibrillation in 2 cases, requiring electrical cardioversion.

Figure. QTc interval prolongation and an episode of polymorphic ventricular tachycardia are observed.
The biochemical parameters showed low serum potassium concentrations in 2 cases, whereas calcium and magnesium levels were normal in all patients. In addition, various toxic substances were detected in urine.
The echocardiogram showed severe biventricular dysfunction in 1 of the patients; ventricular function was normal in all others. After methadone was discontinued and magnesium sulfate, isoproterenol perfusion, and potassium supplements were started, polymorphic ventricular tachycardia disappeared within 7 hours of admission. After 2-3 days, methadone treatment was resumed at the usual doses, with the QTc interval progressively returning to normal in 3 cases; the fourth patient requested voluntary withdrawal before the study was completed.
DISCUSSION
Methadone has been widely used for the treatment of heroine addiction and chronic pain for more than 3 decades. It is generally well-tolerated, has few adverse reactions, and until recently its cardiac effects were unknown. In fact, in 2001 the U.S. Food and Drug Administration discontinued drug surveillance of methadone therapy, considering it safe, and recommended that heroine dependence treatment with this drug be expanded and made more flexible.5 Although some experts do not include methadone treatment as a cause of QT interval prolongation1 and others only consider this possibility to be improbable,4 several cases of polymorphic tachycardia have recently been reported in association with high-dose methadone treatment.6,7
Experimental studies have found that methadone can affect numerous cardiac function parameters through various mechanisms. The stimulation of opiate receptors has a negative chronotropic effect, a phenomenon known to be a predisposing factor for TdP. In addition, in vitro methadone inhibits the rectifying current of the 3 potassium I channels (HERG) or Ikr current, prolonging the action potential of the cardiac cells and consequently, the QT interval.8 The latter is the same mechanism that explains the acquired QT interval prolongation caused by administration of other drugs.1,4 Consistent with these results, later clinical studies have shown that initiation of methadone treatment in patients addicted to heroine is followed by significant QT interval prolongation.9
Among HIV-infected patients receiving antiretroviral therapy and high doses of methadone Gil et al7 reported 4 cases of QT interval prolongation with TdP in 3 of them. Antiretroviral therapy, in particular, protease inhibitors such as nelfinavir, can cause important pharmacological interactions with methadone by inducing or inhibiting the CYP3A4 isoenzyme of cytochrome P450, through which it is metabolized. Concomitant administration of nelfinavir and methadone can result in important changes in plasma concentrations of the latter, possibly leading to the onset of withdrawal symptoms or to intoxication.
As occurred with most patients in earlier studies,6,7 our patients presented some associated risk factors related to QT interval prolongation, for instance, hypopotassemia, intake of drugs that affect the duration of the QT interval, and/or the presence of structural heart disease. The first and third patients had hypopotassemia and were also taking benzodiazepines at high doses. The second was taking methadone doses well above those recommended, with inconstant values due to interaction with the antiretroviral therapy and self-medication. In addition, he presented severe ventricular dysfunction and was being treated with gabapentin, as occurred with one third of the patients in the study conducted by Krantz et al.6 Methadone treatment was continued in all our cases, and suppression of the triggering factors was what led to normalization of the QT interval and disappearance of arrhythmia.
In conclusion, methadone should be included among the drugs that can produce QT interval prolongation and TdP. The risk-benefit ratio of this treatment should also be assessed before combining it with other drugs that prolong repolarization or interfere with their metabolism. In this case, the QTc interval duration should be monitored before and after combined treatment, as well as when high doses of methadone are prescribed, and treatment should be discontinued in case of that induce prolongations of QTc interval duration >500 ms.1,4
Received January 22, 2004.
Accepted for publication February 3, 2005.
Correspondence: Dra. J. Almendral Garrote.
Servicio de Cardiología. Hospital Gregorio Marañón.
Dr. Esquerdo, 46. 28007 Madrid. España.
E-mail: almendral@medifusion.com