
Ablation strategies for pulmonary vein isolation in patients with atrial fibrillation have become both faster and safer in recent years. New devices have also been developed to facilitate a crucial step in the procedure: transseptal puncture for left atrial access.1,2
Our hospital was the first in Spain to use the AcQCross Qx device (Medtronic, USA) for left atrial access. This device has an integrated dilator and needle, which can be used for conventional mechanical puncture or radiofrequency puncture for difficult septa. Because the AcQCross Qx dilator is used to introduce the FlexCath Advance Steerable Sheath (Medtronic) to help position the cryoablation catheter, the system can be simultaneously used to perform transseptal puncture and advance the sheath into the left atrium, simplifying the overall procedure and removing the need for conventional transseptal puncture using a separate sheath and needle system. In the traditional approach, the sheath bearing the needle is exchanged for the deflectable cryoablation sheath-dilator assembly, which is then advanced over the guidewire into the left atrium. The single-step AcQCross Qx approach simplifies left atrial access, reducing both procedure time and the risks associated with sheath exchange. Regardless of the technique used to guide transseptal access (fluoroscopy or ultrasound), once the AcQCross Qx-FlexCath assembly is positioned in the fossa ovalis, the integrated needle is extended by sliding the button on the handle of the AcQCross Qx (figure 1). Because the needle has a more tapered end than a conventional transseptal needle, crossing is achieved without the need for force. The lumen is also sized to accommodate a high-support guidewire, enabling femoral access without predilation and facilitating passage of the dilator and deflectable sheath through the puncture site. This is extremely useful when working with very rigid septa, as a smooth passage can sometimes be difficult to achieve. The few studies that have evaluated the AcQCross-Qx device in clinical practice have demonstrated its safety and efficacy, with reports of a 50% reduction in both transseptal access times for supraventricular left side tachyarrhythmia ablation3 and cryoballoon ablation times.4
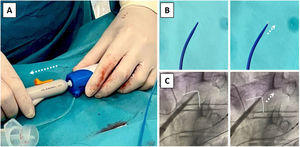
 on the handle of the device is pushed forward to extend the needle from the dilator to the puncture site. B: detailed view of the distal end of the dilator showing the extension of the needle on sliding the button forward. C: radiologic image showing the moment of the puncture. Note the tenting of the fossa ovalis in the first image and the needle crossing the septum in the second.")
AcQCross Qx device for left atrial access. A: AcQCross Qx integrated dilator/transeptal puncture needle system attached to the FlexCath cryoablation sheath. The slider button (arrow) on the handle of the device is pushed forward to extend the needle from the dilator to the puncture site. B: detailed view of the distal end of the dilator showing the extension of the needle on sliding the button forward. C: radiologic image showing the moment of the puncture. Note the tenting of the fossa ovalis in the first image and the needle crossing the septum in the second.
To evaluate the use of the AcQCross Qx in clinical practice, we conducted a retrospective observational study of 20 patients with paroxysmal or persistent atrial fibrillation scheduled to undergo cryoballoon ablation for pulmonary vein isolation between February and April 2023. Transseptal puncture was performed using a conventional approach in 10 of the patients and the integrated AcQCross Qx system in the other 10. The study was approved by the ethics committee at our hospital and informed consent was obtained from all patients.
The 20 patients (13 men; mean±SD age, 59±8 years) were randomized in a 1:1 ratio to the conventional transseptal puncture group or the AcQCross Qx group. We excluded patients with patent foramen ovale detected by transesophageal echocardiography prior to the procedure (table 1). We studied left atrial access times defined as the time from initiation of the transseptal puncture (the moment at which the puncture system is drawn down from the superior vena cava) to insertion of the FlexCath cryoablation sheath into the left atrium. This time reflects the specific usefulness of the device, as it exclusively measures the time required to access the left atrium (ie, it is not influenced by other aspects of the procedure or the preparation of catheters not used for access). The first puncture attempt was successful in 9/10 patients in the AcQCross Qx group and in 7/10 patients in the conventional transseptal puncture group. Mean left atrial access time was 3.34minutes in the AcQCross Qx group vs 5.49minutes in the conventional group (P=0.02). The respective median [interquartile range] access times were 2.39[2.31] minutes and 5.28 [2.33] minutes. Radiofrequency was not needed to achieve puncture in any of the cases. All the procedures were uneventful and there were no puncture-associated complications.
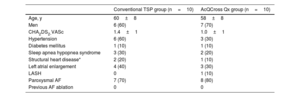
Baseline characteristics of the study population
| Conventional TSP group (n=10) | AcQCross Qx group (n=10) | |
|---|---|---|
| Age, y | 60±8 | 58±8 |
| Men | 6 (60) | 7 (70) |
| CHA2DS2-VASc | 1.4±1 | 1.0±1 |
| Hypertension | 6 (60) | 3 (30) |
| Diabetes mellitus | 1 (10) | 1 (10) |
| Sleep apnea hypopnea syndrome | 3 (30) | 2 (20) |
| Structural heart disease* | 2 (20) | 1 (10) |
| Left atrial enlargement | 4 (40) | 3 (30) |
| LASH | 0 | 1 (10) |
| Paroxysmal AF | 7 (70) | 8 (80) |
| Previous AF ablation | 0 | 0 |
AF, atrial fibrillation; CHA2DS2-VASc, acronym for congestive heart failure; hypertension, age ≥ 75 y (double score), diabetes mellitus, stroke (double score) vascular disease, age 65-74 y, and sex (female); LASH, lipomatous hypertrophy of the interatrial septum; SAHS, sleep apnea hypopnea syndrome; TSP, transseptal puncture.
Values are expressed as mean±SD or No. (%).
The AcQCross Qx device met our expectations: it significantly reduced sheath-cryoablation catheter advancement times, providing a fast and simple solution for left atrial access with zero exchanges. With time and more experience with different puncture techniques, the AcQCross Qx may become part of cryoballoon ablation procedures for atrial fibrillation.
FundingThis study received no funding.
Authors’ ContributionsAll the authors contributed significantly to this study. They were all involved in study design, data collection and analysis, and manuscript preparation. All the authors critically reviewed the manuscript and approved its final version.
Conflicts of InterestNo conflicts of interest related to this article.