To the Editor,
The finding of a small rounded mass over an undiseased valve, with no signs of endocarditis, points to the diagnosis of fibroelastoma. Given the high degree of suspicion provided by these types of images, some authors are in favor of a watchful waiting approach. However, fibroelastomas do not always present in this way, and decision making can be complex.
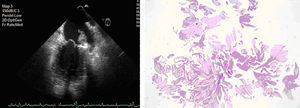
We present 2 cases of presentation at an atrial site. The first corresponds to a 76-year-old man who was admitted for a first episode of heart failure. He had no constitutional or infectious signs and symptoms. Severe mitral valve regurgitation was apparent in the transthoracic echocardiogram. The transesophageal study showed prolapse affecting scallops 2 and 3 of the posterior leaflet. In addition, a homogeneous mobile mass of 1×2cm was found by chance, located on a broad pediculum, adhered to the atrial endocardium and close to the mitral annulus (Figure 1). Neither the valve nor the atrial appendage was involved, but both were increased in size and free of masses. The patient underwent mitral repair and the mass was excised. Pathological examination revealed a 2cm fragment of pearl-colored, “villiferous”-looking tissue. Under the microscope, this form appeared as an avascular papillary tumor with multiple digitiform fronds comprised of dense connective tissue with low cellularity over a matrix of mucopolysaccharides, elastic fibers, and spindle cells, all covered by a layer of hyperplastic endocardial cells (Figure 1).

Figure 1. Long-axis transesophageal image of the left ventricle, in which a mass is observed adhered to the atrial endocardium, contiguous to the mitral annulus. On the right, histological image with hematoxylin-eosin staining, in which the papillary nature of the tumor can be observed.
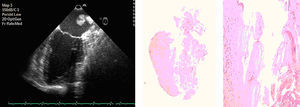
The second case corresponds to a 55-year-old woman with no prior relevant history who was referred for a finding of atrial mass during gastroenterological endoscopy. Transesophageal echocardiography showed a highly mobile mass of 2.5cm, with a broad stalk, adhered to the posterior endocardium of the left atrium, which was of normal size and morphology (Figure 2). Although the patient was asymptomatic, the tumor was removed given its large size and mobility; the pathology report revealed similar histological characteristics to those described for the first case (Figure 2).

Figure 2. Transesophageal 2-chamber image in which the anchoring of the mass to the posterior endocardium of the left atrium, close to the pulmonary veins, can be observed. The histological image also shows anchoring to the atrial endocardium and the villiferous form.
Papillary fibroelastoma was described by Yater in 1931.1 It is the third most common cardiac tumor after myxoma and lipoma, and the one that most frequently affects the cardiac valves.2 There are many theories about its origin: organized thrombus, hamartoma, hyperplastic reaction to external agents, or a form of chronic viral endocarditis.3 Most tumors remain asymptomatic, and so their prevalence is underestimated. In the left-side chambers, they may present as systemic embolism, with cerebral ischemia being the most frequent;4 right-side embolism is less frequent although acute pulmonary embolism or chronic pulmonary hypertension may occur.3
The preferred site is the endocardiac valve, accounting for 75% of cases, and the aortic valve, with no preference for which side, is the most widely affected, followed by the mitral valve (atrial side) and to a lesser extent the tricuspid and pulmonary valves.3 At these sites, the tumors are usually rounded and small. The presence in the image of these characteristics, without any signs of endocarditis, leads to a strong suspicion of fibroelastoma. However, approximately one-fourth of the cases are anchored to the nonvalvular endocardium and the left ventricle is the most frequently affected site. In echocardiography, these tumors show up as mobile digitiform masses, with several villous structures originating from a stalk anchored to the endocardium. Involvement of the endocardial surface of the left atrium accounts for 1.5% to 9.5% of cases in different series,3, 4 and the tumors are small, usually <1cm. Our cases presented with a similar echocardiographic appearance: lobulated, highly mobile, homogeneous masses >2cm, with a broad stalk, adhered to the endocardium of the left atrium. These atypical characteristics of papillary fibroelastoma required a differential diagnosis, essentially with a thrombus (unlikely in the absence of emboligenic structural heart disease) and with atrial myxoma. Given the similarities of our cases, we propose that the finding of a cardiac mass with the echocardiographic characteristics described above, and in the absence of emboligenic heart disease, provided diagnostic suspicion of papillary fibroelastoma at an atypical site.
Four years separated diagnosis of the 2 cases. Since 2000, 13 cases of echocardiographic suspicion of fibroelastoma have been included in our database. Apart from the 2 cases described here, the remaining 11 had a typical site and typical characteristics. Only 3 tumors were resected, and diagnosis of fibroelastoma was confirmed in 2. The 8 remaining patients are undergoing regular follow-up with imaging techniques.
When embolism is diagnosed, the whole tumor tends to be removed to avoid embolic recurrences. There is less agreement for asymptomatic tumors. If the mass is large and mobile, there is consensus about surgical resection if valve replacement is not necessary. However, in cases of typical valve location, small size (1cm), and lack of excessive mobility, watchful waiting with anticoagulation therapy is considered appropriate.3
These recommendations do not, however, apply for fibroelastomas at atypical sites. The reasonable approach when faced with such masses is to rule out as many diagnoses as possible by noninvasive means. Gradual enhancement of magnetic resonance data may help in tumor diagnosis.5 Once diagnosed, surgical resection (provided the risk is not too high) can provide an indication of etiology, prognostic evaluation, and specific treatment.
.
Corresponding author: Semdoc@hotmail.com