To the editor,
Bronchopleural fistulas are an infrequent but very serious complication after pneumonectomy and are associated with high morbidity and mortality.1 Surgical repair is complex and there is little experience in sealing this type of fistula using bronchoscopy with different materials. Early sealing of the fistula is essential because if delay leads to empyema, surgical drainage and prolonged treatment with antibiotics will be required. We report the case of a 75-year-old man who underwent left pneumonectomy for squamous cell carcinoma, followed by radiotherapy and chemotherapy. Nineteen days later he presented with fever, cough with whitish sputum, and subcutaneous emphysema in the left lateral neck region. Bronchopleural fistula was diagnosed and treatment was begun with intravenous meropenem, with good results. During admission, the fistula was sealed by bronchoscopy (Hystoacril®) and the patient was discharged after 11days.
At 20days, the patient presented at the emergency room with fever, malaise, and bronchorrhea. It was confirmed that the fistula had reopened and, as empyema was suspected, the patient underwent open thoracostomy to drain the pleural cavity. He was discharged 1 month later requiring daily care of the thoracostomy site. In a joint session involving the pulmonology, thoracic surgery, and interventional cardiology departments, the possibility of performing a hybrid procedure to implant an Amplatzer® device to seal the fistula was discussed.
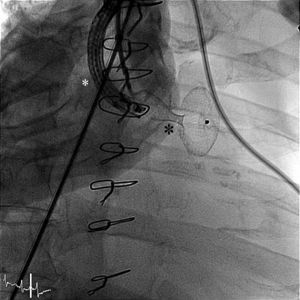
The procedure was performed under sedation in the cardiac catheterization laboratory. First, bronchoscopy was used to assess the size of the fistula, which was found to have a diameter of approximately 10mm. It was decided that the appropriate device would be a 15mm Amplatzer® Septal Occluder, commonly used to close patent foramen ovale. A 0.035” Teflon guidewire was introduced into the fistula through the bronchoscope and was placed distally to the left pleural cavity. Due to the impossibility of introducing a 7 Fr catheter (essential for the device) through the bronchoscope channel, this was withdrawn and the Teflon guidewire was left in the previously described position. The 7 Fr catheter was introduced via the guidewire until the distal tip was located within the pleural cavity. The bronchoscope was reintroduced parallel to the catheter to verify correct placement. Finally, the Amplatzer® device was introduced by fluoroscopy until the distal disk was located in the pleural cavity and the proximal disk inserted into the bronchus to seal the fistula (Figure 1).

Figure 1. Fluoroscopic image of the left thorax. The bronchoscope can be observed (white asterisk) as well as the Amplatzer® device, which is expanded and still attached to the delivery system (black asterisk).
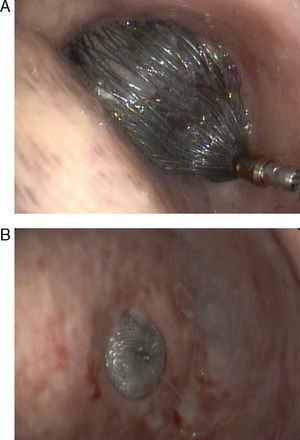
Fiberoptic bronchoscopy within the bronchus and pleural cavity was used to verify that the device was correctly positioned (Figure 2). Fluoroscopy time was 3min and contrast injection was not required. The patient was discharged 48h later without further incident.

Figure 2. A: endobronchial image of the device sealing the fistula and still attached to the delivery system. B: detailed view showing the device closing the fistula and the visceral pleura.
The versatility of percutaneous techniques has been demonstrated recently in a wide spectrum of cardiovascular diseases traditionally handled by other specialists. Several of these techniques involve non-cardiology specialties such as cardiovascular or vascular surgery, which means that hybrid procedures are becoming increasingly important.
Although this technique has been described in some isolated cases,2, 3 we present the first report in Spain of a hybrid procedure involving pneumology, thoracic surgery, and interventional cardiology to resolve a postoperative fistula.
In this case, closure using an Amplatzer® was proposed as an alternative after closure by bronchoscopy with a tissue sealant had failed, as published elsewhere.2 Nevertheless, this could become a first-line technique in this condition as experience with the procedure is gained. One case has already been described in which the technique was used as the first-line option3; in patients like ours who have previously received chemotherapy and radiotherapy, and in whom surgery may be more complex, it is even more justified to consider it as a first-line option.
In short, this technique can provide a solution to complications stemming from other medical and surgical specialties and is an example of the possibilities offered by hybrid procedures between various specialties and different techniques.
Corresponding author: jgoicolea@hotmail.com