
To the Editor,
We present the case of a 78-year-old woman who was admitted to our service with a diagnosis of anteroseptal myocardial infarction. Angiography revealed severe stenosis of left main coronary artery and a critical lesion in proximal left anterior descending coronary artery. Following successful percutaneous revascularization of these lesions, the patient, who was stable and asymptomatic, was transferred to the coronary care unit. A few hours later, she began to have repeated episodes of ventricular fibrillation (VF). She was treated with beta blockers and amiodarone and underwent deep sedation, orotracheal intubation and implantation of an intraaortic balloon pump for counterpulsation. Despite all these measures, it was not possible to control the electrical storm, and external defibrillation was necessary on more than 100 occasions during the first 12h.
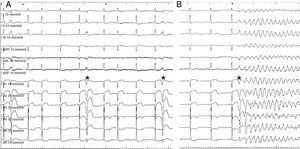
Although this complication occurred over the weekend, given the instability of the patient the decision was made to discuss the case with the electrophysiology team. Upon reviewing the results of the telemetric study, we observed that each episode of VF began with a monomorphic premature ventricular complex (PVC) (Figure 1), with a QRS width of only 120ms. Thus, suspecting that the VF episodes were produced by Purkinje fibers damaged by myocardial ischemia, we decided to perform an emergency electrophysiological study (EPS).

Figure 1. A, high-density monomorphic premature ventricular complex (asterisks). B, the premature ventricular complexes induce repeated ventricular fibrillation episodes.
Following puncture of the femoral artery, we gained access to the left ventricle via a retrograde approach using a 4-mm ablation catheter Marirn® (Medtronic Inc., Minneapolis, MN, USA). During the EPS, the patient continued to have episodes of VF initiated by the same PVC. The earliest activation during the PVC occurred in the anterolateral portion of left ventricle, and we observed a fast potential that preceded the initiation of the QRS complex by 15ms in the electrocardiogram, coinciding with a sharp downstroke in the unipolar lead (Figure 2). The same high-frequency potential was recorded at this point during sinus rhythm and was therefore interpreted as corresponding to activation of the Purkinje fibers.

Figure 2. A, a Purkinje potential (red arrow) precedes the premature ventricular complexes by 15ms. This same potential is observed in the sinus beats (blue arrows). B, a premature ventricular complex preceded by a Purkinje potential induces ventricular fibrillation.
Radiofrequency was applied in this region and the ectopic activity and VF completely disappeared. The patient had no further episodes of VF during the remainder of the hospital stay. However, she died one month later of heart failure.
Ventricular fibrillation following myocardial infarction can be caused by a number of mechanisms. As in the case we present, it can be secondary to PVC generated by activity triggered in the Purkinje fibers of the infarcted region. In experimental models, it has been shown that the Purkinje fibers located in the subendocardium can survive transmural infarctions. When these PVC are frequent and cause an electrical storm, they can be localized by activation mapping and their ablation can resolve the electrical storm.1 In any case, in the presence of an electrical storm produced by VF during the subacute phase of a myocardial infarction, the initial approach should be medical treatment (beta blockers, amiodarone, or other antiarrhythmic agents) and assessment of the need for sedation (including general anesthesia) and implantation of an intraaortic balloon pump for counterpulsation,2 as was done in our patient. Another possible cause of postinfarction electrical storm is recurrent myocardial ischemia, and coronary angiography should be repeated at the slightest suspicion of its presence. In our case, there was no evidence of myocardial ischemia and the presence of monomorphic PVC triggering each episode of VF led us to perform the EPS following the failure of medical treatment. In cases of electrical storm induced by VF, ablation should be indicated only if these PVC are identified and are frequent. Maneuvers to provoke PVC (isoproterenol, provocation of ventricular ectopy) are not effective. Stimulation mapping could be useful if a 12-lead electrocardiographic recording of the PVC could be obtained. Although few cases are reported in the literature, ablation proved to be effective in most of them, always taking into account the fact that this is a complex procedure that should be carried out in centers experienced in ventricular tachycardia ablation.1, 2, 3 It is important to point out that ablation should not be delayed in a patient with electrical storm induced by VF that is suspected to be due to activity triggered in Purkinje fibers, and in some cases it may be necessary to perform the EPS during the off hours of the electrophysiology laboratory, a circumstance that we could consider an “electrophysiological emergency or alert”. In fact, had these measures been taken even earlier in the case we present, we could have avoided a great number of the electrical cardioversions required by the patient, which almost certainly contributed to the deterioration of her myocardial function and to her ultimate death due to heart failure.
.
Corresponding author: jesushernandezh@gmail.com