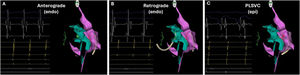
A 37-year-old man with a history of failed ablation for orthodromic tachycardia mediated by a concealed accessory pathway (AP) was scheduled for an electrophysiological study. During the initial study, a persistent left superior vena cava (PLSVC) was incidentally identified. The AP was mapped during tachycardia to the supero-posterior mitral annulus (MA) but ablation was again unsuccessful despite extensive anterograde and retrograde attempts (figure 1A,B).

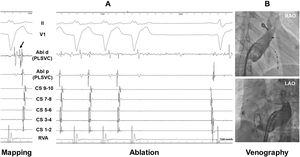
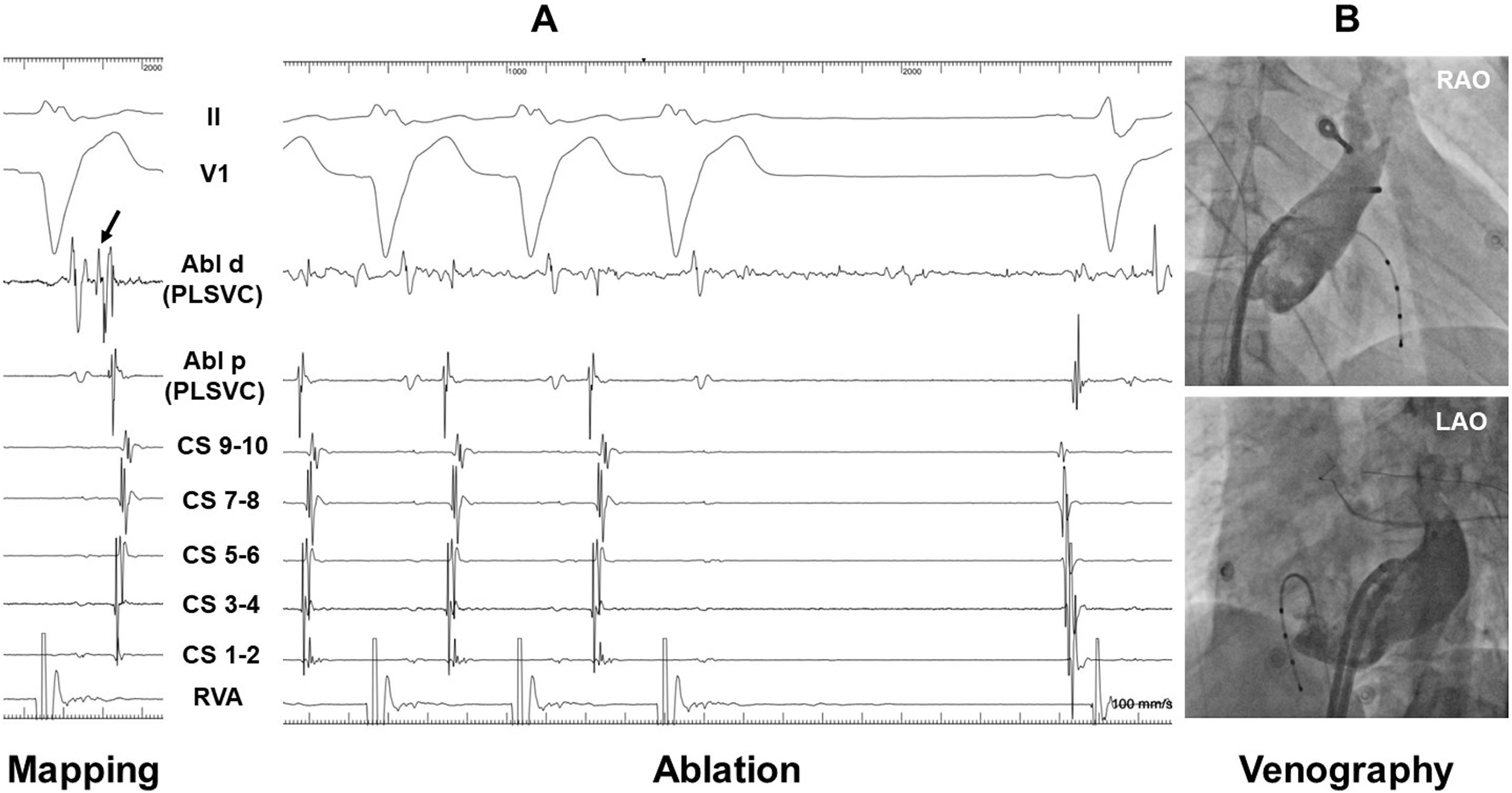
The ablation catheter was then placed within the PLSVC and mapped to a position directly opposite the best endocardial site (figure 1C), with a comparable local ventriculo-atrial interval albeit with a possible Kent-potential visible (figure 2A, arrow; Abl, ablation catheter; CS, coronary sinus; LAO, left anterior oblique; RAO, right anterior oblique; RVA, right ventricular apex). Ablation at this site terminated the tachycardia within 5seconds. Venography confirmed a ventricular position of the ablation catheter within the PLSVC at the supero-posterior MA (figure 2B).

PLSVC is a remnant of the left cardinal vein and is the most common thoracic venous anomaly. We hypothesize that successful epicardial ablation of the AP was facilitated by the presence of the PLSVC, which provided access to the MA. This allowed ablation at a depth where left-sided APs traverse the epicardial fat pads, ie, ablation was not performed at the atrial or ventricular insertions of the AP but rather at the epicardial aspect of the MA, with the PLSVC acting as an ablation vantage point.
Another possibility is that the PLSVC itself harbored AP muscular tracts, which are commonly observed in inferior and infero-paraseptal APs. Although the procedural indication was strong, ablation within the CS/PLSVC elevates the risk of coronary artery damage and perforation. Therefore interventional cardiologist back-up is recommended in such cases.
FUNDINGNo funding was received relevant for this work.
ETHICAL CONSIDERATIONSInformed consent was obtained and archived for the publication of the case. The possible variables of sex and gender, according to the SAGER guidelines, have taken into account.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCENo artificial intelligence was used in the preparation of this paper.
AUTHORS’ CONTRIBUTIONSF. Åkerström drafted the text of the manuscript and F. Åkerström and A. Paul-Nordin drafted the images included. F. Åkerström and A. Paul-Nordin critically reviewed and approved the manuscript.
CONFLICTS OF INTERESTNone.