
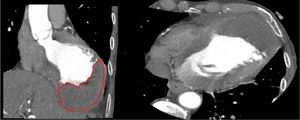
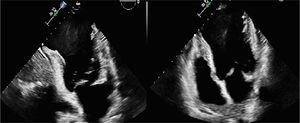
A 78-year-old man, who was an active smoker, presented with a 2-week history of chest pain, dyspnea and orthopnea. On examination, he was tachypneic and had bilateral basal crepitations. Chest X-ray showed bilateral alveolar edema, and blood tests revealed raised troponin and NT-proBNP. Electrocardiogram showed ST elevation in V1 to V5 and Q waves, compatible with acute pulmonary edema secondary to acute evolving anterior myocardial infarction. Transthoracic echocardiogram (figure 1, ) showed a dilated left ventricle with a large dyskinetic apical region with a hyperechoic image within it (8×6 cm), indicative of intraventricular thrombus, and a left ventricular ejection fraction of 25%. Computed tomography (figure 2) showed a large apical thrombus in the left ventricle (3.1×6.2×9.6cm) occupying at least 50% of the cavity.


After finding some cases in the literature of intraventricular thrombus treated with direct oral anticoagulants (DOACs), the medical team decided to start anticoagulation with apixaban 5 mg/12h.
The patient progressed well. One month after discharge, repeat echocardiogram showed no thrombus but persistence of the large apical aneurysm with slow flow through it (figure 3, ).

Although the usual treatment is with heparin or vitamin K antagonists and there are no randomized clinical trials with DOACs, this case demonstrates the effectiveness of apixaban in resolving a large intraventricular thrombus in 6 weeks. Informed consent was obtained prior to publication.
FUNDINGNone.
AUTHORS’ CONTRIBUTIONSG.M. Heredia Campos wrote the case report. J. Perea Armijo was responsible for the investigations. M. Anguita Sánchez had a supervisory role.
CONFLICTS OF INTERESTNone.
Supplementary data associated with this article can be found in the online version available at https://doi.org/10.1016/j.recesp.2021.11.008