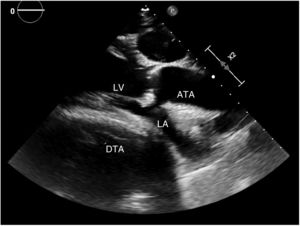
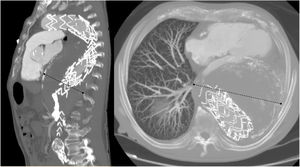
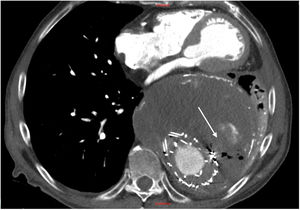

The present case concerns a 77-year-old man who attended our emergency department due to frank hemoptysis. Seven years ago, he underwent an intervention involving a fenestrated endovascular stent graft due to a ruptured thoracoabdominal aortic aneurysm. Multiple reinterventions were required due to persistent endoleaks and progressive growth of the aneurysm sac in the descending thoracic aorta, which reached 15cm in size (figure 1; ATA, ascending thoracic aorta; DTA, descending thoracic aorta; LA, left atrium; LV, left ventricle). Given the high surgical risk and the technical impossibility of definitive endovascular treatment, the patient was under follow up by vascular surgery. Six months ago, he began experiencing dyspnea on minimal exertion (New York Heart Association [NYHA] II-III) and mild and intermittent hemoptysis. Echocardiography revealed a major change in cardiac geometry due to a large aneurysm sac pressing on the left posterior ventricular wall and atrium (figure 2). Systolic function was preserved but there were signs of significant diastolic dysfunction, with increases in ventricular and pulmonary artery filling pressures. At admission, physical examination showed no signs of heart failure and electrocardiography demonstrated normal sinus rhythm with no ST segment changes. His hematocrit was 37%. Thoracoabdominal computed tomography angiography revealed an increase in the size of the aneurysm sac (to 17cm), compression of the left branch of the pulmonary artery, and a marked alteration of the cardiac anatomy due to compression of the left atrium. In addition, gas was visible in the interior of the aneurysm sac, indicating the presence of an aortobronchial fistula (figure 3, arrow). Given the elevated morbidity and mortality of open surgery, a conservative strategy was adopted. The patient's consent was obtained for publication of the case.
FUNDING


The present work has not received funding.
Authors’ ContributionsS. González Sánchez reviewed the data, wrote the article, and selected the images. M. Herrero Gutiérrez participated in the manuscript drafting and figure design. I.M. Breteau Agote participated in the manuscript drafting and data collection.
CONFLICTS OF INTERESTNo conflicts of interest.