We present the case of a 59-year-old patient with no cardiovascular risk factors and a medical history only remarkable for multiple episodes of cutaneous lipomatosis. He was seen for progressive effort angina of 6-months' evolution. The physical examination, electrocardiogram, general analyses and chest x-ray were normal, and the early stress test showed positive clinical and electrocardiographic signs and electrical monitoring. Echocardiography showed normal heart valves and left ventricle, and revealed a partially calcified tumor mass in the posterior left atrioventricular groove, that protruded noticeably over the posterior mitral annulus, without causing hemodynamic stenosis in the mitral valve. Computed tomography and chest magnetic resonance imaging confirmed the presence of a tumor (diameter, 45 mm) with the radiological characteristics of a lipoma and internal areas of calcification and liquefaction.
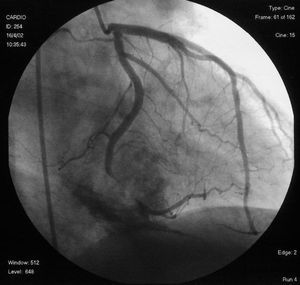
Coronary angiography showed angiographically normal coronary arteries, with the exception of significant extrinsic compression of the circumflex artery in the posterior atrioventricular groove, secondary to the tumor and generating 95% stenosis (Figure). The patient was treated surgically with resection of the capsulated posterior subepicardial tumor mass, which freed the circumflex artery. Abundant lipid-caseous material drained from the mass and histological study identified a lipoma with areas of necrosis, liquefaction and calcification. Culture and stains for bacteria and fungi were negative.

Fig.
The postoperative period was unremarkable, and the patient remains asymptomatic at 1 year of follow-up, with no radiological evidence of tumor or myocardial ischemia on stress testing.