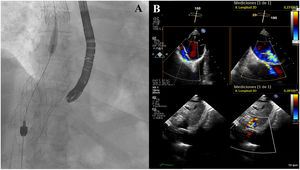

A 71-year-old man with massive tricuspid regurgitation was admitted with peripheral edema and ascites, gaining up to 15kg in weight, despite intensive diuretic treatment (furosemide 160mg, spironolactone 50mg, and hydrochlorothiazide 25mg). The Heart Team decided on caval valve implantation (CAVI) with TricValve (Products & Features, Austria)—superior 29mm, inferior 41 mm— as the patient was not a candidate for edge-to-edge repair and was considered to be at high risk for surgery due to extreme obesity. The outcome of this first procedure was good, with prosthesis deployment slightly down and minimal residual leak (< 3 mm) (figure 1A,B).

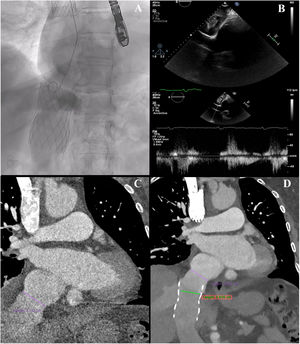
After being asymptomatic for 1 year, the patient was referred for right heart failure symptoms. Echocardiography showed dilated suprahepatic veins and inferior cava venous and preserved right ventricle function (TAPSE 20mm), with mean pulmonary pressure 23mmHg and pulmonary vascular resistance 0.88 uW. Atrial angiography showed significant regurgitation to the inferior vena cava due to prosthesis migration as computed tomography similar diameter of inferior cava concerning previous (figure 2A-D).

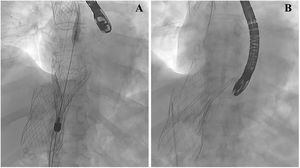
A second TricValve 41mm prosthesis was considered the best option (CAVI-in-CAVI). Under general anesthesia and fluoroscopy and transesophageal echocardiography (TEE) guidance, it was implanted inside the previous prosthesis successfully sealing the transition from the inferior caval vein to the right atrium (figure 3) (). The patient was discharged the day after the procedure without complications. One month later, he was still feeling well and has lost 8kg.

To the best of our knowledge, this is the first tricuspid CAVI-in-CAVI procedure to resolve prosthesis migration. The patient's consent was obtained for this publication.
FUNDINGNone.
AUTHORS’ CONTRIBUTIONSS. López-Tejero and P. Antúnez-Muiños, contributed equally to the conception, design, and drafting of this paper. I. Cruz-González headed this project and approved the final version. The corresponding author accepts responsibility for this article.
CONFLICTS OF INTERESTI. Cruz-González is proctor for Products and Features.
Supplementary data associated with this article can be found in the online version, at https://doi.org/10.1016/j.rec.2022.09.010