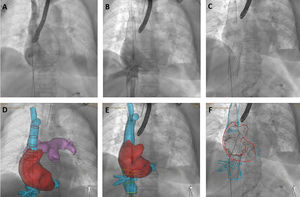
Severe isolated tricuspid regurgitation is seldom treated surgically. Percutaneous tricuspid valve intervention options include heterotopic caval valve implantation (CAVI) in both caval veins. In this procedure, the valve system can be mounted on a single drug-eluting stent placed between the 2 caval veins (Tricentro, NVT, Switzerland) or on 2 separate supports (TricValve, Products&Features, Germany). Patient selection and the choice of bioprosthesis size rely on computed tomography (CT) reconstruction. The procedure usually involves the use of selective angiography to place a catheter in the right pulmonary branch and another catheter or guidewire at the transition toward the inferior caval vein (figure 1A,B).

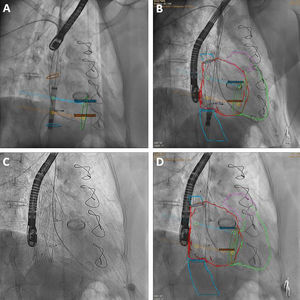
Our group has explored the use of CT-fluoroscopy fusion imaging (HeartNavigator 3.0, Philips, the Netherlands) with the placement of specific markers to guide bicaval valve implantation in 6 consecutive patients (2 with the Tricentro valve and 4 with the TricValve system). For the Tricentro valve, CT-fluoroscopy visualized the cavoatrial junctions and neovalve orientation (figure 2A,B); for the TricValve devices, the procedure showed the same measurements and heights as the screening (figure 1D,E). In our experience, CT-fluoroscopy provided accurate imaging support for CAVI, improving the identification of anatomical features and permitting a scan arc orthogonal to the landing zone. CT-fluoroscopy also allowed the pigtail catheter to be withdrawn before valve deployment. This prevents the catheter becoming trapped, maintains reference points, and allows the detection of unnoticed catheter malpositioning in the pulmonary branch (catheter positioning above or below the target zone reduces implantation accuracy, and CT-fluoroscopy helps to avoid this by revealing the artery edges and volume). This imaging approach could also reduce the number of selective angiograms and the amount of contrast agent used; however, these outcomes were not assessed in this initial analysis. The final outcome can be seen by comparing figure 1C,F and figure 2C,D.
