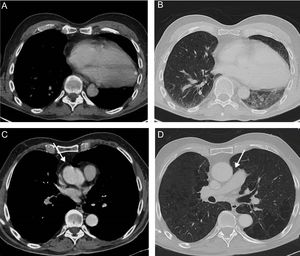
We describe the case of a patient who was incidentally diagnosed with an asymptomatic cardiac herniation on a positron emission tomography/computed tomography (PET/CT) scan performed for staging purposes after a chest radiograph detected a mass in the right lung. The patient had been involved 27 years earlier in a high-energy motor vehicle accident and suffered a severe traumatic head injury as well as multiple bone fractures, from which he had recovered after a long hospital stay. Since the patient was discharged 27 years previously, he had had no cardiac symptoms except for some intermittent palpitations. The CT component of the PET/CT study showed classic findings of cardiac herniation secondary to a ruptured pericardium, including a left heart deviation with clockwise rotation of the cardiac apex (Figure A, asterisk), secondary atelectasis of the left lower lobe (Figure B, asterisk), pericardial discontinuity (Figure C, arrow), and interposition of lung tissue between the ascending aorta and the main pulmonary artery (Figure D, arrow) due to the absence of the pericardial layer; PET/CT confirmed locally advanced lung cancer.

Posttraumatic cardiac herniation (PTCH) is a rare and life-threatening condition associated with a high mortality rate and usually requires emergency surgery. Most patients with PTCH become symptomatic within 24hours following trauma; however, the diagnosis of PTCH may be delayed in patients with a sufficiently large pericardial tear to permit free herniation of the heart without great vessel strangulation, as probably occurred in our patient. To our knowledge, no PTCH has previously been diagnosed such a long time after severe thoracic blunt trauma.