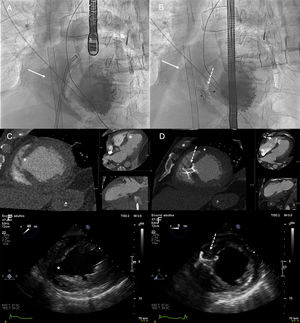
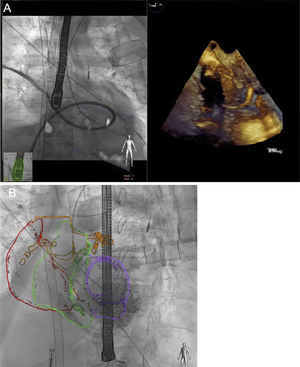
A 75-year-old man was admitted due to acute myocardial infarction complicated by cardiogenic shock. A coronary angiogram showed proximal left anterior descending artery occlusion; a transthoracic echocardiogram revealed severe left ventricular dysfunction and a ventricular septal rupture (VSR). Extracorporeal membrane oxygenation (ECMO) and intra-aortic balloon pump were implanted and left anterior descending percutaneous coronary intervention was performed. After discussion, the decision was made to perform transcatheter VSR closure on ECMO. A 22-mm postinfarct ventricular septal defect Amplatzer device (Abbott) was successfully implanted. Figure 1A and 1B show fluoroscopy, computed tomography (Figure 1C, 1D) and transesophageal echocardiography (Figure 1E, 1F) images before and after closure (arrow: ECMO cannula; dotted arrow: postinfarct ventricular septal defect device; asterisk: VSR). Figure 2 shows sheath crossing of the VSR (echocardiographic-fluoroscopic fusion) and the final result with Heart Navigator (overlay of the computed tomography 3-dimensional reconstructions on live fluoroscopy). Two days later, a minimal residual shunt and left ventricular function recovery were reported. Consequently, the ECMO and intra-aortic balloon pump were removed without complications.


Early surgical repair is recommended for VSR, but common practice is to delay surgery and many of these patients are not treated. Published data suggest there is increasing use of ECMO in patients with VSR complicated by cardiogenic shock as a bridge to surgical repair. However, to the best of our knowledge, this is the first reported case of successful VSD transcatheter closure on ECMO. The hemodynamic stabilization achieved with ECMO could permit a meaningful delay in VSR closure in patients with cardiogenic shock, allowing scar tissue formation around the defect and reducing intervention risk.
CONFLICTS OF INTERESTI. Cruz-González is proctor for Abbott.