An epsilon wave on a 12-lead electrocardiogram is an important diagnostic criterion for arrhythmogenic right ventricular dysplasia. This delayed right ventricular depolarization manifests as low amplitude electrical potentials between the end of the QRS complex and the beginning of the T wave, most prominently in leads V1 to V3. The epsilon wave is detected in 30% of individuals with arrhythmogenic right ventricular dysplasia; however, the epsilon wave can be masked by excessive low-pass filtering, and the true rate may therefore be higher.
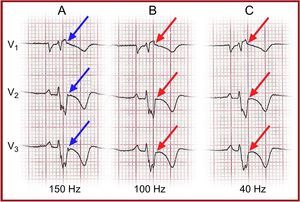
The Figure shows how low-pass filter cutoff frequency influences the detection of the epsilon wave in arrhythmogenic right ventricular dysplasia: At the recommended 150Hz cutoff frequency (Figure A), the epsilon wave is detected in leads V1-V3. At a 100Hz cutoff frequency (Figure B), the epsilon wave is attenuated in V1-V2 and absent in V3. At 40Hz (Figure C), the epsilon wave disappears from leads V1-V3.

The low-pass filter cutoff frequency needs to be optimally adjusted to ensure that important clinical information is not lost (the QRS complex and its notches, the J wave and the pacemaker spike). Current electrocardiography guidelines set the cutoff at 150Hz for adolescents and adults. Nonetheless, in routine clinical practice a 40Hz cutoff frequency is used to reduce muscle noise and improve the appearance of the trace.
This practice results in the loss of important information, leading us to conclude that the presence of an epsilon wave in patients with arrhythmogenic right ventricular dysplasia may be seriously underestimated.