
The subcutaneous implantable cardioverter-defibrillator (S-ICD) was introduced to reduce complications related to the transvenous leads used with conventional defibrillators. The device has proven to be a safe and effective system for both primary and secondary prevention of sudden cardiac death.1,2
The S-ICD creates an extrathoracic defibrillation system by means of subcutaneous defibrillation leads placed along the sternum and tunneled through the subcutaneous inframammary line to a generator located in the chest wall. However, in patients with pectus excavatum, it may be difficult to position the lead around the convexity formed by the left chest and the concavity located around the sternum.
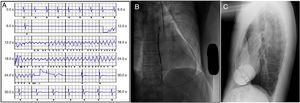
We describe a 41-year-old man who was resuscitated following cardiac arrest due to ventricular fibrillation during physical exercise. The patient had no relevant history, although pectus excavatum (Figure 1A) was observed during the physical examination. In the cardiac study performed, no significant abnormalities were found in either the electrocardiogram or echocardiogram. Coronary angiography showed no coronary abnormalities. Cardiac magnetic resonance imaging revealed fibrosis in the septal segments of the left ventricle, as well as severe pectus excavatum (Haller index, 9.5) (Figure 1B).
 and cardiac magnetic resonance image (B) showing pectus excavatum.")
In view of the diagnosis of recovered ventricular fibrillation and the possibility of arrhythmogenic cardiomyopathy, ICD therapy was indicated for secondary prevention of sudden cardiac death.
An S-ICD was initially considered because pacing was not required and there was no indication for cardiac resynchronization, based on the patient's age and clinical arrhythmia (lower probability of requiring antitachycardia pacing).
Electrocardiographic screening was positive for the 3 vectors in the left parasternal position. Because screening was successful, the risks of a subcutaneous vs conventional device were evaluated, with assessment of the impact of the chest deformity on subcutaneous lead insertion, detection of ventricular electrical activity, and defibrillation efficacy. Finally, a decision was made to implant an S-ICD (Emblem MRI S-ICD A219).
Implantation was carried out under local anesthesia with conscious sedation. Even though a 2-incision technique with no cranial incision was used, the single-coil defibrillation lead was successfully placed in a conventional position. The generator was positioned laterally between the anterior surface of the serratus muscle and the latissimus dorsi, behind the anterior axillary line. After implantation, ventricular fibrillation was induced and successfully reverted by the S-ICD with a shock of 65J (safety margin, 15J) (Figure 2A) and defibrillation impedance of 42Ω. The primary sensing vector was programmed (proximal lead to can), and 2 detection zones were also programmed: a conditional zone at 200 bpm and a shock zone above 250 bpm. There were no complications following the procedure, and proper positioning of the lead and generator were confirmed by chest radiography (Figure 2B-C).
, posteroanterior chest radiography (B), and lateral chest radiography (C) following placement of a subcutaneous implantable cardioverter-defibrillator.")
At the 3-month follow-up visit, the patient was asymptomatic, the incisions had healed properly, and device interrogation revealed no arrhythmic events.
The S-ICD is a valid alternative to transvenous ICD, and several prospective registries have shown similar safety and efficacy for the 2 devices.1,2 Further experience with S-ICD use has been gained in recent years in aspects related to therapy indication, implantation techniques, and device programming. In Spain, the S-ICD accounts for 5% of all ICD devices implanted.3 The S-ICD has obvious advantages for younger patients with indications for an ICD, as a way to prevent complications associated with the use of transvenous leads.
This report is the first description of S-ICD implantation through a 2-incision technique in a patient with pectus excavatum. While it is conceivable that a chest deformity could limit the use of S-ICD, in our patient there was no impact on electrocardiographic screening, defibrillator lead placement, detection of induced ventricular fibrillation, or shock effectiveness. In other published cases, a 3-incision technique was employed,4 showing that implantation is feasible in these patients. Our report provides further evidence of the efficacy of a simpler surgical procedure with a shorter implantation time.2 The outcome achieved in our patient suggests that the S-ICD can be used in individuals with chest deformities when it is clinically suitable and electrocardiographic screening is successful.