A 75-year-old woman with Child B primary biliary cirrhosis under treatment with ursodeoxycholic acid was hospitalized for edematous ascitic decompensation related with spontaneous bacterial peritonitis, which was treated with intravenous ciprofloxacin. On the third day, she had an onset of anginal pain, anterior wall ST-segment elevation, and cardiogenic shock.
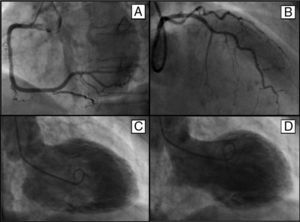
Urgent catheterization showed an absence of significant coronary lesions (Figures 1A and B) and severely depressed systolic function, with medial and apical dyskinesia of the anterior and inferior walls, and hypercontractility of the basal segments (Figures 1C and D), consistent with tako-tsubo syndrome. The patient received inotropic support and underwent implantation of a counterpulsation balloon, but she died at 12hours due to multiorgan dysfunction and consumption coagulopathy.

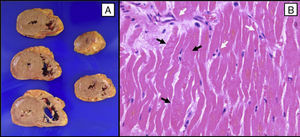
The post mortem macroscopic study showed an absence of structural changes (Figure 2A). Microscopy revealed contraction bands in the myocardial fibers (Figure 2B, black arrows) and diffuse infiltration of polymorphonuclear leukocytes (Figure 2B, white arrows) throughout the left ventricle.

The pathological findings of endomyocardial biopsies described in tako-tsubo syndrome include interstitial infiltrates of lymphocytes, leukocytes and macrophages, myocardial fibrosis, and contraction bands, with or without myocyte necrosis. The inflammatory changes and contraction bands differentiate tako-tsubo syndrome from the coagulation necrosis occurring in acute myocardial infarction. This is a singular case because postmortem study enabled examination of the entire heart, which confirmed that the reported microscopic findings are diffusely present in all the left ventricular territories.