Examination of a 22-year-old man with a 10-year history of moderate exertional dyspnea revealed perioral cyanosis, finger clubbing, oxygen saturations of 81%, and a grade III/IV systolic murmur in the pulmonary area. Electrocardiography and echocardiography showed right ventricular hypertrophy. Echocardiography also showed isolated infundibular pulmonary stenosis (IIPS) with a maximum gradient of 106mmHg and an intact interventricular septum.
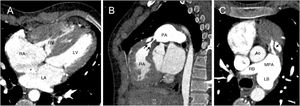
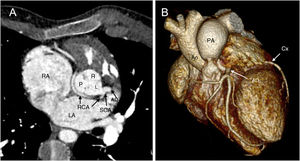
Computed tomography angiography showed a 21-mm ostium secundum atrial septal defect (figure 1A, asterisk; RA, right atrium; LA, left atrium; RV, right ventricle; LV, left ventricle), right ventricular hypertrophy with IIPS from muscular bands (figure 1B,C, arrows; Ao, aorta; PA, pulmonary artery; RB, right branch; LB, left branch; MPA, main pulmonary artery), a normal pulmonary valve, a 20-mm pulmonary annulus, and dilatation of the MPA and its left branch. A single coronary artery (SCA) was detected arising from the left coronary sinus and giving rise to the right coronary artery (RCA), with a retroaortic course toward the left main stem (figure 2; R, right coronary sinus; L, left coronary sinus; P, posterior sinus).


Dilatation of the MPA is not typical in IIPS. It has been suggested that this could be due to MPA wall stress caused by high velocity flow generated in the infundibulum.
The patient was referred for surgery, during which the pulmonary valve was confirmed to be normal.
IIPS is very rare (around 0.09%-2% of all congenital heart defects) and its association with a single coronary artery is even less common, with only 1 case reported.