
Interrupted aortic arch is a congenital malformation characterized by a complete separation between the ascending aorta and the descending aorta. In type B interrupted aortic arch, the most common form of the condition, the separation is produced between the left carotid and subclavian arteries and is associated with an interventricular communication. The descending aorta is supplied by the pulmonary artery through a patent ductus arteriosus.
We present the case of an 8-year-old boy with type B interrupted aortic arch. The physical examination was remarkable for a single, strong second heart sound, secondary to pulmonary hypertension, and asymmetric pulses, which were stronger in the right arm and both carotids than in the other limbs. The patient also presented differential cyanosis with clubbed fingers of the left hand and toes of both feet.
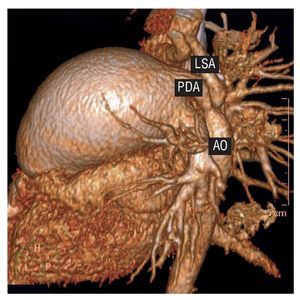
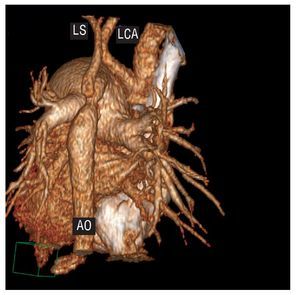
Angiographic reconstructions of images obtained with a 64-slice multidetector computed tomography unit, performed with a low-dose radiation protocol (80 kV, 50 mA), show anterior (Figure 1), lateral (Figure 2), and posterior (Figure 3) views. The main pulmonary artery (MPA) is severely dilated because of the pulmonary hypertension. The origin of the left carotid artery (LCA), which receives oxygenated blood from the ascending aorta, is clearly differentiated from that of the left subclavian artery (LSA) and the remainder of the descending aorta, which is supplied by the pulmonary artery with mixed blood because of the presence of a ventricular septal defect with left-to-right shunting. The patent ductus arteriosus (PDA) is restrictive, which explains the asymmetric pulses.

Figure 1.

Figure 2.

Figure 3.
ABBREVIATIONS
LCA: left carotid artery
LSA: left subclavian artery AO: aorta
MPA: main pulmonary artery PDA: patent ductus arteriosus