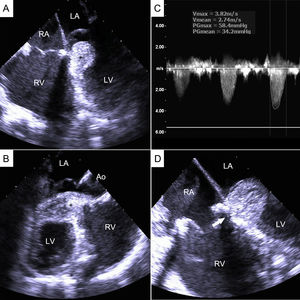
A 15-year-old boy with severe Ebstein anomaly underwent corrective surgery. Considered a poor candidate for cone repair due to extensive tethering of the anterior leaflet and a vestigial posterior leaflet, the patient underwent bioprosthetic tricuspid valve replacement with extensive plication of the atrialized right ventricle (RV). Surgery was uneventful and routine transesophageal echocardiography was performed upon weaning from extracorporeal circulation. Bioprosthetic function was adequate without paravalvular leaks. However, a previously unknown mass was noted on the left side of the interventricular septum (Figure A, asterisk; LA, left atrium; LV, left ventricle; RA, right atrium). This mass was of similar echodensity to the myocardial wall, had a smooth surface, and was adherent to the interventricular septum, making even more remote the hypothesis of a thrombus. It also protruded into the LV outflow tract (Figure B, ; Ao, aorta), causing significant obstruction (Figure C; mean gradient of 34mmHg) at this early stage of weaning from extracorporeal circulation. Closer inspection revealed a saccular arrangement of the mass, following an inflection point in the right ventricular side (Figure D and ; arrow). This finding demonstrated that the mass was indeed a plicate portion of the interventricular septum following the wave of plication performed on the atrialized RV. This plication was completely redone from the RA with a good result. Despite being previously unreported, this strictly mechanical complication should be suspected when complex Ebstein corrective surgery with atrialized cavity reduction is pursued.
ISSN: 1885-5857
Impact factor 2024
4.9
