A 45-year-old, male, previous smoker was admitted for exertional stable angina pectoris that had started 8 months before, with Tc-99m-single photon emission computed tomography evidence of partially reversible inferior ischemia.
The patient underwent coronary angiography, which revealed a total occlusion in the proximal segment of the right coronary artery, with collateral circulation from septal branches of the left anterior descending.
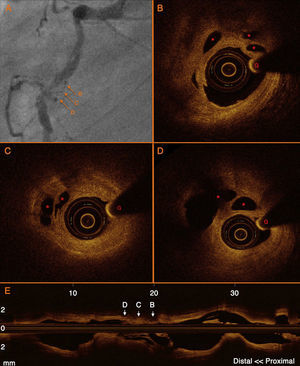
The occlusion could be easily crossed using a tapered Fielder XT® wire supported by an over-the-wire 2mm balloon. The dilatation restored sufficient flow to allow an optical coherence tomography (OCT) examination performed with a DragonFlyTM catheter and C7 LightLab, St. Jude Medical system with pull-back at 2cm/s during automatic contrast injection at 3mL/s. Numerous microchannels within a large, positively remodeled fibrotic plaque were observed in the initially occluded segment of the mid-right coronary artery (Figure). With OCT images we are able to differentiate true microchannels from dissection after predilatation (microchannels have no contact with true lumen, no communication between them, and no evidence of solution of continuity).

Chronic total occlusions consist of mixed fibro-atheromatous plaque and thrombus depending on the mechanism of occlusion and its duration (by definition more than 3 months). Over time endothelialized microchannels with a diameter between 0.08 and 0.26mm develop within the thrombotic component and often traverse the occlusion for long segments and facilitate progression of soft, low-profile, polymer-coated guidewires. This is the first image reported, to our knowledge, of microchannels studied in vivo taking advantage of the superior resolution of OCT.