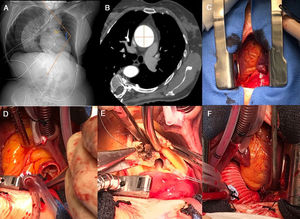
We present the case of a 56-year-old woman, (height 141cm, weight 50kg), hypertensive, with severe right congenital kyphoscoliosis and short neck (figure 1A, X-ray: right severe kyphoscoliosis with a Cobb angle of 79°). She presented dyspnea (New York Heart Association class II) 1 year ago. Physical examination revealed a systolic murmur. Transthoracic ultrasound showed severe aortic stenosis due to a bicuspid valve, with normal ventricular function and moderate pulmonary hypertension. Computed tomography exposed a tortuous thoracic aorta due to severe kyphoscoliosis and aortic aneurysm 46 x 47mm, without sinus dilation of Valsalva (figure 1B). Respiratory functional tests showed a restrictive disorder: forced vital capacity of 1.87L and forced expiratory volume in the first second of 68%.

Mechanical aortic valve prosthesis and supracoronary graft replacement were performed by ministernotomy in J through third right intercostal space, under extracorporeal circulation (figure 1C-F). The patient was extubated 4hours after surgery without analgesic supplements. Total chest drainage was 500mL. Postoperative course, supported by early respiratory physiotherapy, was uneventful.
Severe spine deformities reduced lung capacity and cause restrictive respiratory and heart failure. The smaller sternal incision causes less pain and restriction of respiratory dynamics in patients with impaired lung function. As in this patient, ministernotomy is associated with shorter intubation time, less postoperative bleeding, and shorter hospital length stay. However, individualized decision-making is required to minimize potential complications.