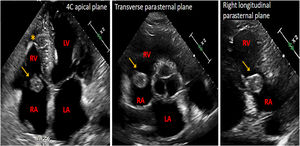
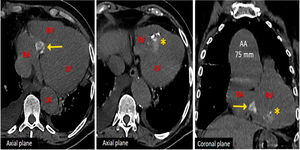
A 70-year-old woman presented with chest pain. Transthoracic echocardiogram revealed the presence of a severe uncomplicated aneurysm of the ascending aorta (diameter of 75mm) and a solid tricuspid rounded tumor (diameter of 20mm) with a hypercoic contour. The tumor appeared to be dependent on the posterior leaflet implantation (figure 1, arrow; RV: right ventricle; RA: right atrium; LV: left ventricle; LA: left atrium), but valve function remained unaltered. Laboratory parameters showed no abnormalities, and coronary angiography showed normal results. Computed tomography confirmed the presence of an aortic aneurysm (figure 2A) and revealed calcification within the tricuspid tumor (figure 2, arrows), which extended into the interventricular septum and the right ventricle (RV) wall (figure 2, asterisk).


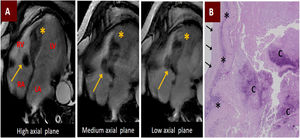
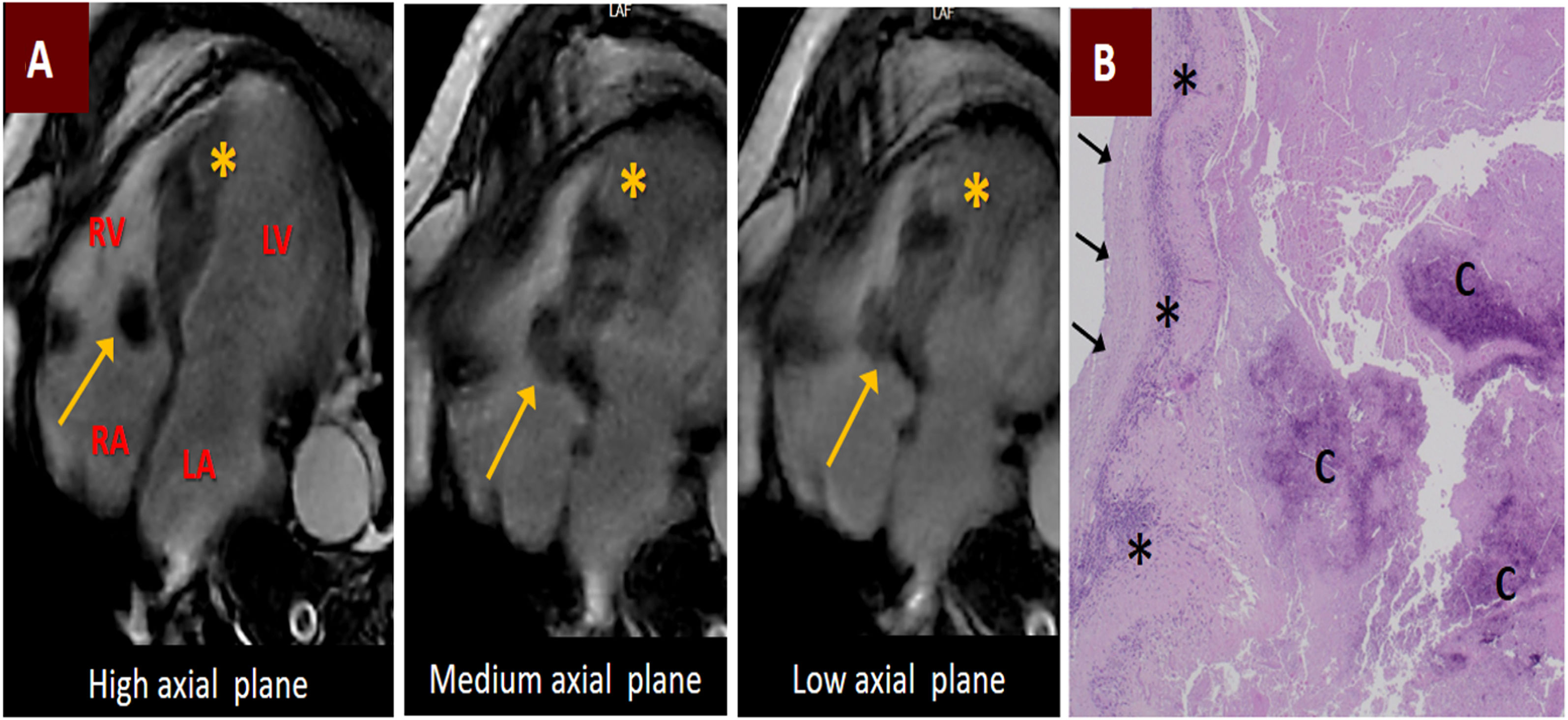
Magnetic resonance imaging demonstrated a sessile mass at the tricuspid annulus, located at the level of the septal leaflet (figure 3A, arrows), with intramyocardial extension towards the intraventricular septum and RV wall (figure 3A, asterisk). The mass exhibited hypointensity on T1-weighted images and showed no enhancement, either initially or after gadolinium administration. The patient subsequently underwent replacement of the ascending aorta and aortic valve (Bentall procedure), excision of the mass, and repair of the tricuspid valve using a pericardial patch.

Macroscopically, the mass was composed of whitish, toothpaste-like encapsulated material. Microscopic examination revealed necrotic, proteinaceous material with calcifications (figure 3B,C), an inflammatory infiltrate (figure 3B, asterisk), and a fibrous capsule (figure 3B, arrows). Diagnosis of caseous calcification and necrosis of the tricuspid annulus with intramyocardial extension was confirmed. Unfortunately, the patient experienced severe bleeding complications during the postoperative period and died. Due to this unexpected and fatal outcome, as well as the inability to contact the patient's family, we were unable to obtain informed consent to report the images for this case. However, the images were appropriately anonymized. This is the second reported case of caseous tricuspid annulus necrosis, but is the only report with a histologically-confirmed diagnosis.
FUNDINGNothing to disclose.
AUTHORS’ CONTRIBUTIONSD.I. Gentille Lorente: clinical management of the patient, performance of the echocardiography, manuscript conception, literature review, manuscript drafting and composition of images, submission of the manuscript to the journal. V. Pineda Sánchez: interpretation of magnetic resonance images, literature review, collaboration in writing the manuscript.
CONFLICTS OF INTERESTNothing to disclose.