
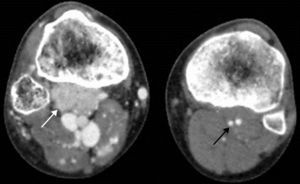
The patient was a 21-year-old man with a lifelong history of skin lesions (well-defined port wine stains) on the right thigh, which had exhibited progressive growth, accompanied by pain and ulceration. Physical examination revealed hypertrophy of the right lower extremity and venous varicosities, with an ischemic ulcer in the medial malleolus. There was a palpable thrill and audible murmur in the dorsum of the foot. Computed tomography angiography was performed in the abdomen and lower extremities, and 3-dimensional reconstructions (Figure 1) showed a marked increase in the lumen of the right iliofemoral artery territory (black arrows) compared with the left side (black arrowhead), and early venous filling in the right iliofemoral territory (white arrow); there were numerous varicosities throughout the affected extremity. At the level of the proximal tibial metaphysis, in the posterior compartment of the right leg (Figure 2), axial images showed more intense staining in the popliteus muscle than in the remainder of the proximal musculature (white arrow) and left popliteus muscle (black arrow), relative to the arteriovenous malformation nidus.


Parkes-Weber syndrome is characterized by high-flow arteriovenous fistulas, and the most serious complication is heart failure; although its etiology is unknown, this syndrome has been associated with a mutation of the E133K gene of angiogenic factor VG5Q, which controls the growth of blood vessels (angiogenesis), and is transmitted by autosomal dominant inheritance.
The case we report here coincides with the clinical data and imaging findings associated with this syndrome (increased volume of the affected lower extremity, cutaneous vascular changes, and high-flow arteriovenous fistulas).