
A 55-year-old woman with a 3-year history of precordial pain was diagnosed with Takayasu arteritis (TA) at age 30 that manifested as the absence of left radial pulse, claudication of the upper limbs, and hypertension.
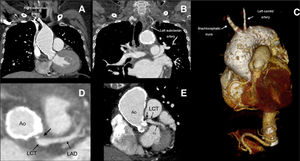
Computed tomography showed ascending aorta dilatation and extensive circumferential calcification from the aortic annulus and involving the ascending aorta, aortic arch, supra-aortic vessels (brachiocephalic trunk and left carotid artery), and segments of the descending aorta (figure 1). The scan also revealed occlusion in both subclavian arteries and in the right carotid artery (figure 2A-C) and partially calcified plaque in the ostium of the left coronary trunk (LCT), with stenosis <50% (figure 2D-E, arrow; Ao, aorta; Cx, circumflex artery; LAD, left anterior descending artery).


Porcelain aorta is extensive circumferential calcification of the thoracic aorta. It is classified as type I when it affects the ascending aorta regardless of extension and is subdivided into type IA when there is no possibility of aortic clamping during cardiac surgery and type IB when aortic clamping is possible but with greater risk. Porcelain aorta is classified as type II when only located in the aortic arch or the descending aorta.
Although aortic calcification in Takayasu arteritis has already been reported, this case is of interest due to the presence of very severe calcification and type IA porcelain aorta. Informed consent was obtained from the patient for publication.
FUNDINGNone.
AUTHORS’ CONTRIBUTIONSD.I. Katekaru-Tokeshi compiled the data, interpreted the cardiac computed tomography images, and wrote the article. M. Jiménez-Santos reviewed the cardiac computed tomography images and provided a critical review of the article. Both authors approved the final version.
CONFLICTS OF INTERESTNone declared.