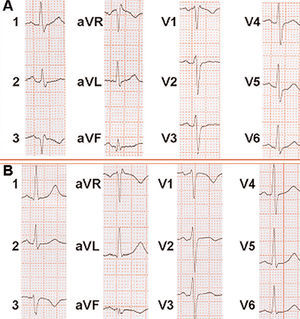
A 52-year-old man was seen in the emergency room for syncope and dyspnea. He had no cardiological history of interest and had been immobile for some time due to a right ankle injury with a fibular fissure; prophylactic antithrombotic treatment was not undertaken. On examination, the patient was found to have tachycardia and tachypnea, with no other findings. The hemogram, biochemistry analyses, and chest x-rays were normal. Blood gas analysis showed hypoxemia with hypocapnia, and the electrocardiogram revealed sinus tachycardia with a typical SI QIII TIII pattern and complete right bundle branch block (Figure 1A).

Fig. 1.
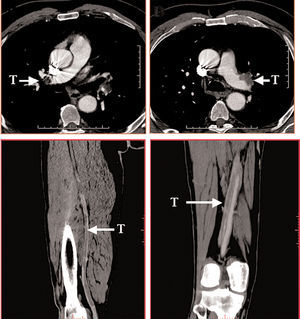
On the basis of suspected pulmonary thromboembolism, multislice computed tomography (CT) with intravenous contrast was performed. A pulmonary embolism affecting the two main pulmonary arteries with progression to the three lobar branches on the right side and to the inferior lobe on the left was visualized (Figure 2A and B). With the same dose of contrast material administered, the study was extended to the venous system of the lower limbs, which showed extensive thrombosis of both deep femoral and popliteal veins (Figure 2C and D).

Fig. 2.
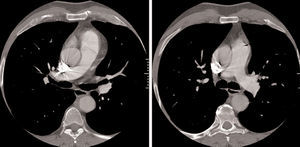
The patient became asymptomatic after administration of fibrinolytic treatment, and the SI QIII TIII echocardiographic pattern and right bundle branch block disappeared (Figure 1B). Follow-up CT showed total resolution of the pulmonary embolism (Figure 3A and B).

Fig. 3.