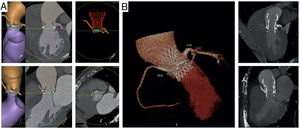
A 76-year-old man was admitted with heart failure secondary to a failed 25-mm Mitroflow (Sorin Group USA Inc, United States) valve with severe aortic regurgitation and reduced left ventricular ejection fraction. The Heart Team decision was to perform a valve-in-valve procedure (ViV) with pre-emptive positioning of stents in the left main (LM) and right coronary artery (RCA). A preprocedural computed tomography scan enabled us to identify anatomical features (5.7mm LM height, 8.5mm RCA height and shallow sinuses of Valsalva with a valve distance to coronaries <4mm) associated with increased risk for coronary compromise during ViV (figure 1A; ).

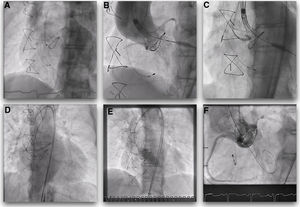
During valve deployment, the patient experienced acute hypotension and complete atrioventricular block due to RCA obstruction. Consequently, the stent was withdrawn and deployed with immediate hemodynamic normalization. The CoreValve (Medtronic, United States) prosthesis was released completely with significant underexpansion. As the Mitroflow leaflet seemed to be displaced close to the LM ostium following CoreValve deployment, an LM stent was deployed as a preventative measure. Valve postdilation was successfully performed using a kissing technique with simultaneous inflation of the aortic balloon and both coronary stent balloons (figure 2; ). At 3 months of follow-up, the patient was in New York Heart Association class I with preserved left ventricular ejection fraction, and a computed tomography scan ruled out stent complications (figure 1B).

Coronary occlusion during ViV is a rare but life-threatening complication. It is also a preventable complication. Guided by periprocedural multimodality imaging, pre-emptive coronary protection enables us to anticipate and prevent coronary occlusion in selected patients at high risk.
Supplementary data associated with this article can be found in the online version available at https://doi.org/10.1016/j.rec.2020.07.011