

A 69-year-old patient, who had received a permanent central venous catheter through the subclavian vein in 2000, presented with 2 syncopal episodes in February 2003. The transthoracic echocardiogram showed a right atrial mass. Transesophageal echocardiography (Figure 1) confirmed the presence of a 27x14-mm mobile mass (arrows) anchored to the atrial wall near the tricuspid annulus by a thick pedicle. The catheter tip was located near the mass, but was not adhering to it. The patient underwent extracorporeal circulating cardiac surgery (Figure 2), in which the atrial mass was resected and the catheter withdrawn. Pathological examination documented a fibrin thrombus with calcifications (Figure 3). Microbiological culture was negative. Six months after the procedure the patient was asymptomatic.

Figure 1

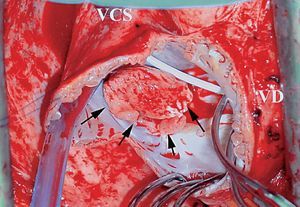
Figure 2

Figure 3.
In adult patients with indwelling venous catheters and no concomitant infection, right atrial thrombus is uncommon and tends to have an asymptomatic course. The thrombi are usually found adhering to the catheter, rarely attached to the atrial wall. It has been suggested that such thrombi are caused by injury to the atrial endocardium produced by the catheter tip. According to some reports, detachment of the thrombus can provoke an embolism or tricuspid valve occlusion. In the case of sessile parietal thrombi, catheter removal and anticoagulant treatment are sufficient. However, resection is indicated for large, pedunculated thrombi.