
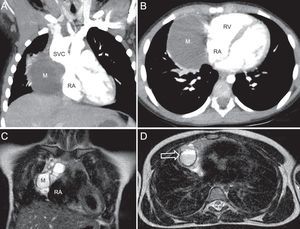
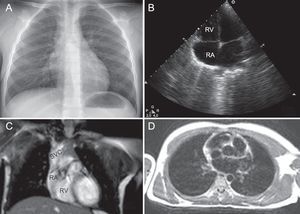
A 6-year old girl with a small right submandibular lymphatic malformation detected when she was 2 year old was admitted with fever, murmur, and suspected right pneumonia (Figure 1A). A large cystic mass (M) was observed on echocardiography, adjacent to the right atrium (RA) (Figure 1B, ; RV, right ventricle). Computed tomographic angiography showed the lesion to be located in the anterior mediastinum, causing aneurysmal dilatation of the superior vena cava (SVC) (Figure 2A) and compression of the RA, which measured 8 x 6 x 6cm (Figure 2B). The nonnodular aspect ruled out enlarged lymph nodes suggestive of lymphoma and there were no calcifications, which are more frequent in thymomas and germ cell tumors. Gadolinium-enhanced magnetic resonance angiography showed poorly defined edges, heterogeneous signal, and multiple cysts of different sizes within the lesion (Figure 2C), with fluid-fluid levels (Figure 2D, arrow) and contrast uptake at the walls. Ultrasound-guided biopsy was performed, and histologic diagnosis of cystic lymphatic malformation was confirmed. Chest X-ray, echocardiography, and subsequent magnetic resonance imaging showed regression (Figure 3A-3D). The patient remained asymptomatic after 4 years of follow-up.



Lymphatic malformations are common congenital vascular abnormalities. Their behavior depends on their site — cervicofacial presentation is most common — and whether they cause vessel or organ compression. They may occasionally bleed and transiently increase in size. Currently, the preferred treatment is conservative or sclerotic with doxycycline or bleomycin. Surgery is reserved for cases with compromised contiguous structures. For inoperable symptomatic cases, oral rapamycin is used.