A 71-year-old man underwent a percutaneous coronary intervention for an occlusive restenosis of a bare-metal stent implanted 7 years before in the left anterior descending coronary artery. The guidewire (Runthrough NS™, Terumo, Tokyo, Japan) passed the target lesion smoothly. After a 1.5-mm balloon dilatation, optical coherence tomography (OCT) images were obtained by using M3× Cardiology Imaging System™ (LightLab Imaging, Inc., Westford, The US), and a 0.019-in. imaging wire (ImageWire™, LightLab Imaging, Inc.) with automatic-pull back at 1mm/s and 20frames/s. An occlusion balloon catheter (Helios™, Avantec Vascular Corp., Sunnyvale, The US) was inflated proximally to the target segment, and the distal vessel was flushed with heparinized Ringer's Lactate. Cypher™ stents (2.5×23mm and 3.0×28mm, Cordis, Miami, The US) were implanted after a 3.0mm balloon dilatation. Thus, this patient was discharged without any complication.
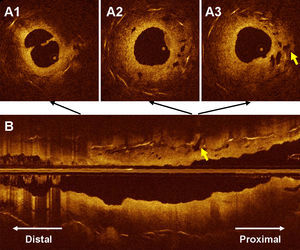
At the restenotic tissue, OCT images revealed the dissection (Figure 1) owing to the balloon dilatation and the microvessels (Figure 1) which are the signal poor structures less than 200 microns in diameter that show a trajectory within the vessel. It has been observed that the microvessels are sometimes visible at OCT images of in-stent restenotic tissue. In this case, microvessels enabled the guidewire to pass the lesion smoothly. However, some of them showed the connection with the extra-stent tissue (Figure 1, arrow). This case reveals the entity of microvessels in occlusive restenotic tissue and the connection of the microvessel with the extra-stent tissue may facilitate the development of subintimal dissections.

Figure 1.
Corresponding author: PXE00364@nifty.com