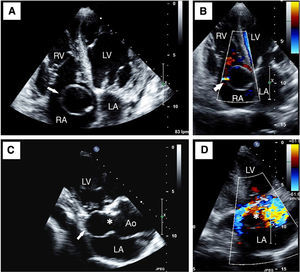
A 93-year-old woman was admitted to our hospital because of dyspnoea at rest, orthopnea, paroxysmal nocturnal dyspnoea and oedema in the lower extremities during the previous four weeks. The physical examination presented rales, elevated jugular venous pressure, hyperkinetic arterial pulse and a pansystolic mild heart murmur. A transthoracic echocardiogram was performed, showing a normocontractile left ventricle (LV), a mildly enlarged and hypokynetic right ventricle (RV), and a mild tricuspid valve regurgitation. In the four-chambers apical level, a well-defined ring-shaped image was visualized inside the right atrium (RA) (arrow, Figure 1A). Careful rotation of the transducer towards a three-chambers apical view allowed us to ascertain that this unusual image corresponded to a huge aneurysmatic enlargement of the non-coronary sinus of Valsalva (arrow, Figure 1C) showing a clear communication between the aneurysm and the aortic lumen (Ao) with the colour Doppler examination (*, Figure 1D). Finally, the abnormal flow from the aortic aneurysm to the right atrium began in systole but extended into diastole, defining a small fistulous communication (arrow, Figure 1B) and distinguishing it from tricuspid regurgitation.

Figure 1.
The final diagnosis was heart failure secondary to right ventricle overload due to left-to-right shunt. The treatment choice for sinus of Valsalva aneurysms that fistulize to other cardiac chambers is surgical correction, but, given the advanced age of the patient, any aggressive treatment was refused, being discharged after compensating her heart failure.
Corresponding author: anapastorplanas@hotmail.com