This article reports the results of the 2020 Spanish Catheter Ablation Registry, a year marked by the SARS-CoV-2 pandemic.
MethodsData were collected retrospectively through completion and return of a specific form by the participating centers.
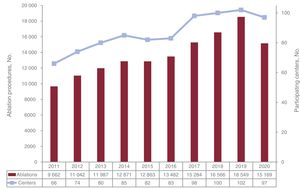
ResultsData from 97 centers (67 public, 30 private) were analyzed. A total of 15 169 ablation procedures were reported with a mean of 155±117 and a median [interquartile range] of 115 [62-227]. Because of the SARS-CoV-2 pandemic, both procedures and participating centers markedly decreased (−3380 procedures,−18%) and there were 5 centers less than in 2019. The most common procedure continued to be atrial fibrillation ablation (4513; 30%), well ahead of the remaining substrates, followed by ablation of the cavotricuspid isthmus (3188; 21%), and intranodal re-entry tachycardia (2808; 18%). Ablation of these 3 substrates continued to form the bulk of the procedures. The total success rate was slightly lower than in previous years (88%) with a similar complication rate (n=309; 2%) and mortality (n=7; 0.04%). A total of 243 procedures were performed in pediatric patients (1.6%).
ConclusionsThe Spanish Catheter Ablation Registry systematically and continuously reflects the national trajectory, which, in 2020, was markedly affected by the SARS-CoV-2 pandemic. Although slightly lower than in previous years, the success rate remained high, with a low complication rate.
Keywords
For 2 decades and without interruption, the Spanish Catheter Ablation Registry, an official report of the Heart Rhythm Association of the Spanish Society of Cardiology, has described the changes over time in the interventional management of arrhythmias in Spain.1–19 The registry aims to provide objective and reliable data on the safety and effectiveness of the ablative treatment of the different ablation targets and on the available facilities and resources in Spanish arrhythmia units. Understandably, the data from 2020 have unfortunately been affected by the SARS-CoV-2 pandemic.
METHODSData collection was retrospectively performed using a standardized form sent to all electrophysiology laboratories in Spain in January 2021. Data submission is voluntary and anonymous, with the secretary of the Spanish Society of Cardiology removing center identifiers.
The registry provides data on the technical and human resources of the participating arrhythmia units and the types of procedures undertaken and their targets, as well as their outcomes and complications. Using the previously established categorization, the arrhythmias and arrhythmogenic substrates were analyzed in 10 categories: atrioventricular nodal reentrant tachycardia (AVNRT), accessory pathways (APs), atrioventricular node (AVN), focal atrial tachycardia (FAT), cavotricuspid isthmus (CTI), macroreentrant atrial tachycardia (MAT), atrial fibrillation (AF), idiopathic ventricular tachycardia (IVT), ventricular tachycardia (VT) associated with myocardial infarction (VT-AMI), and ventricular tachycardia not associated with myocardial infarction (VT-NAMI).
The following variables common to these substrates were analyzed: numbers of patients and procedures (specifying the number of pediatric patients, defined as those younger than 15 years), acute success (at the end of the procedure), type of ablation catheter used, and numbers and types of complications, including periprocedural death. Also analyzed were a number of ablation target-specific variables, such as type, location, and underlying heart disease. The use of electroanatomic mapping systems was also recorded for all procedures, as well as if they were performed without fluoroscopy. As in previous years, the success rate refers to acute success (at the end of the procedure) and the complications recorded are those occurring during the hospital stay. In 2020, given the SARS-CoV-2 pandemic, it seemed pertinent to request additional information in an attempt to quantify the impact of the pandemic on the clinical practice in Spanish laboratories.
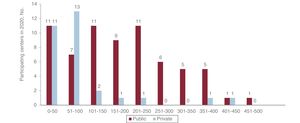
RESULTSThe upward trend of previous years was broken in 2020, both in terms of participation and number of ablations. After reaching a historic high in 2019, the first visible effect of the SARS-CoV-2 pandemic was a slight fall in participating centers (appendix 2). A total of 97 centers participated in 2020 (5 fewer than in 2019, −4%). The second expected effect was the drop in the total number of ablation procedures (figure 1). Specifically, 15 169 procedures were reported in 2020 (3380 fewer than in 2019, −18%). These data are reflected in both the mean (155 ± 117) and the median (115 [interquartile range, 62-227]) per center. In 2020, only 14 centers (2 private) performed more than 300 ablations and 3 (1 private) more than 400. Figure 2 shows the number of procedures per center and the distribution of centers by type of funding.


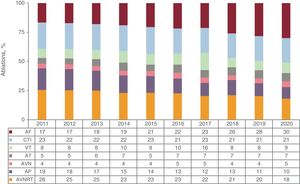
Despite the fall in the number of cases, the ablation target hierarchy has been consolidated, with AF further increasing its distance from the other substrates. AF (4513 procedures) represented 30% of the total (1325 more procedures than the next most commonly treated ablation target). CTI ablation was unchanged (21%) but showed a larger gap vs the third ablation target (AVNRT), which fell to 18%. The numbers for all substrates, without exception, decreased in 2020 but the greatest drop was seen with the paroxysmal supraventricular tachycardias (AVNRT, FAT, and APs), with decreases of about 25%. This affected the total number, given the sheer volume of procedures performed for this type of ablation target. Figure 3 illustrates the changes over time by ablation target.
; AVN, atrioventricular node; AVNRT, atrioventricular nodal reentrant tachycardia; CTI, cavotricuspid isthmus; VT, ventricular tachycardia.")
Changes in the relative frequency of the different ablation targets treated in the last decade. AF, atrial fibrillation; AP, accessory pathway; AT, atrial tachycardia (focal and atypical flutter); AVN, atrioventricular node; AVNRT, atrioventricular nodal reentrant tachycardia; CTI, cavotricuspid isthmus; VT, ventricular tachycardia.
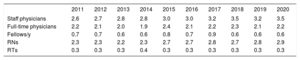
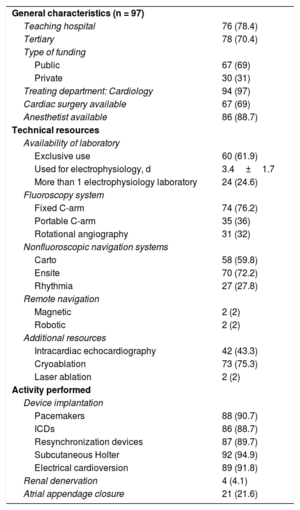
Table 1 and table 2 show the technical and human resources in the participating laboratories, as well as their different activities.
Human resources in Spanish laboratories
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Staff physicians | 2.6 | 2.7 | 2.8 | 2.8 | 3.0 | 3.0 | 3.2 | 3.5 | 3.2 | 3.5 |
| Full-time physicians | 2.2 | 2.1 | 2.0 | 1.9 | 2.4 | 2.1 | 2.2 | 2.3 | 2.1 | 2.2 |
| Fellows/y | 0.7 | 0.7 | 0.6 | 0.6 | 0.8 | 0.7 | 0.9 | 0.6 | 0.6 | 0.6 |
| RNs | 2.3 | 2.3 | 2.2 | 2.3 | 2.7 | 2.7 | 2.8 | 2.7 | 2.8 | 2.9 |
| RTs | 0.3 | 0.3 | 0.3 | 0.4 | 0.3 | 0.3 | 0.3 | 0.3 | 0.3 | 0.3 |
RN, registered nurse; RT, radiologic technologist.
Technical resources and additional activity of participating laboratories
| General characteristics (n = 97) | |
| Teaching hospital | 76 (78.4) |
| Tertiary | 78 (70.4) |
| Type of funding | |
| Public | 67 (69) |
| Private | 30 (31) |
| Treating department: Cardiology | 94 (97) |
| Cardiac surgery available | 67 (69) |
| Anesthetist available | 86 (88.7) |
| Technical resources | |
| Availability of laboratory | |
| Exclusive use | 60 (61.9) |
| Used for electrophysiology, d | 3.4±1.7 |
| More than 1 electrophysiology laboratory | 24 (24.6) |
| Fluoroscopy system | |
| Fixed C-arm | 74 (76.2) |
| Portable C-arm | 35 (36) |
| Rotational angiography | 31 (32) |
| Nonfluoroscopic navigation systems | |
| Carto | 58 (59.8) |
| Ensite | 70 (72.2) |
| Rhythmia | 27 (27.8) |
| Remote navigation | |
| Magnetic | 2 (2) |
| Robotic | 2 (2) |
| Additional resources | |
| Intracardiac echocardiography | 42 (43.3) |
| Cryoablation | 73 (75.3) |
| Laser ablation | 2 (2) |
| Activity performed | |
| Device implantation | |
| Pacemakers | 88 (90.7) |
| ICDs | 86 (88.7) |
| Resynchronization devices | 87 (89.7) |
| Subcutaneous Holter | 92 (94.9) |
| Electrical cardioversion | 89 (91.8) |
| Renal denervation | 4 (4.1) |
| Atrial appendage closure | 21 (21.6) |
ICD, implantable cardioverter-defibrillator.
Values represent No. (%) or mean ± standard deviation.
As in 2019, 61 centers (61%) were equipped with at least 1 dedicated cardiac electrophysiology laboratory. Centers with more than 1 laboratory continued to be a minority: 22 centers had 2 laboratories (22.6%) and 2 centers had 3 (2%). On average, the laboratory was available on 3.4 ± 1.7 (median, 4) days a week (similar to 2019). All centers implanted at least 1 type of cardiac device, although 6 implanted only implantable Holter monitors.
At least 1 fixed C-arm fluoroscopy system was available in 74 centers (76.2%). Only 7 centers had no mapping system (3 private and 4 publicly funded, all except 1 performing fewer than 50 ablations per year); 28% had 2 such systems and 20% had 3. The most common platform was the Ensite system (72.2%). In addition, 32% of centers were equipped with rotational angiography and 43.3% with intracardiac echocardiography. Finally, 75.3% performed cryoablation but laser ablation availability was negligible (in only 2 centers, with no AF ablations reported with this energy source).
The dedicated personnel in the electrophysiology laboratories was unchanged (table 1). Neither were there changes in the number of units training fellows (38%); most had 1 fellow (range, 1-8).
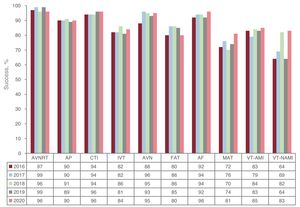
Overall resultsFor the first time since 2015, the success rate fell below 90% (to 88%), although the complication rate was stable (2%). Figure 4 and figure 5 show the success rates and complications reported in recent years by ablation target.
. AF, atrial fibrillation; AP, accessory pathway; AVN, atrioventricular node; AVNRT, atrioventricular nodal reentrant tachycardia; CTI, cavotricuspid isthmus; FAT, focal atrial tachycardia; IVT, idiopathic ventricular tachycardia; MAT, macroreentrant atrial tachycardia; VT-AMI, ventricular tachycardia associated with acute myocardial infarction; VT-NAMI, ventricular tachycardia not associated with acute myocardial infarction.")
Changes in the success rate by ablation target in the last 5 years (no previous success rate data are available for AF). AF, atrial fibrillation; AP, accessory pathway; AVN, atrioventricular node; AVNRT, atrioventricular nodal reentrant tachycardia; CTI, cavotricuspid isthmus; FAT, focal atrial tachycardia; IVT, idiopathic ventricular tachycardia; MAT, macroreentrant atrial tachycardia; VT-AMI, ventricular tachycardia associated with acute myocardial infarction; VT-NAMI, ventricular tachycardia not associated with acute myocardial infarction.

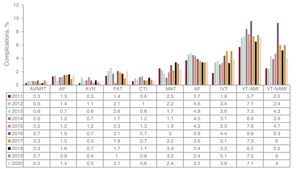
Changes over time in the percentage of complications by ablation target. AF, atrial fibrillation; AP, accessory pathway; AVN, atrioventricular node; AVNRT, atrioventricular nodal reentrant tachycardia; CTI, cavotricuspid isthmus; FAT, focal atrial tachycardia; IVT, idiopathic ventricular tachycardia; MAT, macroreentrant atrial tachycardia; VT-AMI, ventricular tachycardia associated with acute myocardial infarction; VT-NAMI, ventricular tachycardia not associated with acute myocardial infarction.
A total of 309 complications were reported. The most frequent continued to be vascular complications (n = 100) and pericardial effusions/tamponades (n = 93). There were 14 atrioventricular blocks (half in AVNRT and 2 during CTI ablation). Also reported were 2 aortic punctures during transseptal access. Regarding mortality, 7 periprocedural deaths were recorded (0.05%): 4 in VT ablation, 1 delayed death due to septic shock in AF ablation, and 2 of unspecified causes in less complex substrates (FAT and CTI).
The following sections summarize the different ablation targets.
Atrioventricular nodal reentrant tachycardiaAVNRT ablation represented 18% of all procedures (2808 procedures, the third most common ablation target after AF and CTI). This was a highly significant reduction vs 2019, with 960 fewer procedures. This was the ablation target treated in the highest number of centers (n = 95), with an average of 29.3 ± 21 (range, 1-97) procedures/center and a 96% success rate. The most commonly used ablation catheter was the conventional 4-mm catheter (93%). The use of other types of catheters and energy sources was negligible.
The use of nonfluoroscopic navigation systems continued to increase, reaching 31% (from 25% in 2019), and up to 79% of navigation system-guided procedures were fluoroscopy free. The reported complication rate was 0.5%, which included 7 permanent atrioventricular blocks, 3 transient blocks, 1 pneumothorax, and 4 vascular complications.
Accessory pathwaysAP ablation remained the fourth most frequently treated substrate (10%), despite a significant drop in 2020 (1539 procedures vs 2024 in 2019). This ablation target was treated in the vast majority of centers (94 of 97), with an average of 16.2 ± 12.2 (range, 1-54) procedures/center and a 90% success rate. Just 18.2% of the APs showed anterograde conduction exclusively, whereas 39.5% were concealed APs and 42.3% had bidirectional conduction. In addition, left APs continue to not only be the most frequent (47.6%), but also the most successful (98.5%), followed by inferoseptal (29.5%; 92.3% success rate), para-Hisian/anteroseptal (12.1%; 78.4% success rate), and right ventricular free wall (10.8%; 94.7% success rate).
Once again, 4-mm catheters were the most commonly used catheters (57%), followed by irrigated catheters (24%). Contact forcesensing technology continues to gain traction (12.3% in 2020 vs 7.1% in 2019).
Epicardial ablation was performed in 36 procedures and, in the case of left APs, retroaortic access was used in 60%. There were 21 complications (1.4%): 9 pericardial effusions, 8 vascular, 2 embolic phenomena, 1 bilateral pulmonary embolism after left AP ablation, and 1 catheter entrapment in the mitral subvalvular apparatus requiring surgery.
The use of mapping systems continued to grow, reaching almost half of procedures (48.7%), with 35.6% of them performed without fluoroscopy.
Focal atrial tachycardiaIn total, 471 FAT procedures (3%) were reported, with an increase in the number of centers (n = 79) and an 80% success rate. Most (74%) were located in the right atrium, with a 92.2% success rate. In addition, 123 procedures were performed in the left atrium, with a slightly lower success rate (89.1%). The tendency continued for lower use of conventional irrigated tip catheters (144 procedures; 30.5%) due to an increase in contact forcesensing catheters (215 procedures; 45.6%). The data showed a notable increase in the use of mapping systems (71.5%) and 21.4% of the total were performed without fluoroscopy. Ten complications (2%) were reported; the most notable were 3 vascular complications (0.6%) and 4 pericardial effusions (0.8%).
Cavotricuspid isthmusCTI continues to be the second most commonly treated ablation target (3188 procedures; 21%). This substrate was treated in 94 centers, with a mean of 33.9 procedures/center and a mean success rate of 96%. The catheter of choice continues to be the conventional irrigated tip catheter (46.7%), whereas the use of contact forcesensing technology remains the second most common option (27%). The use of 8-mm catheters was unchanged (23.5%). Mapping system use showed a marked increase (42.7%), as well as zero-fluoroscopy interventions (25.2%). A total of 20 complications (0.6%) were reported, including 11 vascular, 2 pericardial effusions, 2 atrioventricular blocks, 1 embolism, and 1 myocardial infarction. One death was reported, but the cause was not specified.
Macroreentrant atrial tachycardiaMAT continues to be one of the least common ablation targets, despite being treated in 73 centers; 582 procedures were reported (4%). The most frequent subtype was that occurring after AF ablation (47.9%). Less frequent were MATs in congenital heart diseases (17.2%) or after arteriotomy (16%). It had the lowest success rate of all procedures (81.4%). The use of mapping systems was stable (81.6%), although there was a slight decrease in zero-fluoroscopy procedures (55 procedures; 9.4%). Contact forcesensing technology (71.9%) predominated over conventional irrigated catheters (10.2%). After AF, it was the supraventricular arrhythmia with the highest complication rate (14 cases; 2.4%); notable complications were 4 femoral vascular complications and 6 pericardial effusions.
Atrioventricular node ablationIn total, 750 AVN ablations (4.9%) were reported by 84 centers. The success rate was 95%. Most of the procedures were performed with conventional 4-mm catheters (399 procedures; 53.2%) or conventional irrigated catheters (212 catheters; 28.3%). The use of 8-mm catheters fell once again (n = 110; 14.6%). Four nonsevere complications were reported (0.5%): 3 vascular and 1 embolism.
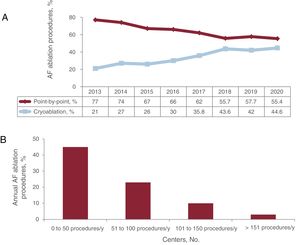
Atrial fibrillationAF became consolidated as the most frequently treated ablation target, with 4513 procedures and increases from 23% in 2017 to 26% in 2018, 28% in 2019, and 30% in 2020. Although the mean number of procedures remained above 50 ablations/center (55.7 ± 44.5), the median was lower (44; range, 1-222). The acute success rate was 96%. Figure 6 shows the distribution of centers by annual AF ablation volume in 2020. Of the 81 centers undertaking AF ablation, 45 (55.5%) performed between 1 and 50 procedures (18 of these centers performed fewer than 25). Just 13 centers exceeded 100 procedures/y (16%), 3 of which performed more than 150 and only 1 more than 200.
.")
Paroxysmal AF ablation comprised 60.8%, persistent AF comprised 33.9%, and long-standing (>1 year) persistent AF comprised 5.1%.
The predominant target continued to be electrical isolation of the pulmonary veins (94.5%) and the data showed a fall in the treatment of other ablation targets (51 fractionated electrogram ablations and 107 superior vena cava isolations). Left atrial lines were placed in 192 procedures (4.3%). Other targets were limited (24 atrial appendage isolations and 8 rotor ablations and ablations of low-voltage areas or extrapulmonary foci).
Although the most commonly used technique continued to be point-by-point radiofrequency (2369 procedures; 55.4%), the use of cryoablation increased (2144 procedures; 44.6%). Figure 6 shows the changes over time in procedures performed with the point-by-point technique vs cryoablation since 2013. In contrast to previous years, the use of other techniques was not reported.
Irrigated catheters with contact forcesensing technology were the catheter of choice (84.8%). Steerable sheaths were reported in 56% of procedures undertaken with radiofrequency. Although 43.3% of centers are equipped with intracardiac echocardiography, it was used in only 18 centers (441 procedures; 9.7% of AF procedures). Six centers reported zero-fluoroscopy procedures (n = 75).
The number of complications was stable (159; 3.5%), with only 1 death, which was attributed to septic shock. In addition, 43 vascular complications were recorded (0.9%), as well as 50 pericardial effusions (1.1%), 35 phrenic nerve palsies (0.7%), and 11 embolisms (0.2%) as the most noteworthy events.
Idiopathic ventricular tachycardiaIn total, 649 IVT ablation procedures were performed in 620 patients, representing 4% (similar to 2019), although there was a notable decrease in the number of procedures vs the 807 in 2019. The number of centers treating this ablation target was unchanged (n = 88), with an average of 7.4 ± 5.8 (range, 1-23) procedures/center and an 83.7% success rate.
Of these, 298 procedures involved VT of the right ventricular outflow tract, 97 involved VT of the left ventricular outflow tract, 64 involved VT of the aortic root, 32 were fascicular tachycardias, 32 were epicardial tachycardias, 4 had an origin in the pulmonary artery, and 72 were in other locations, such as the papillary muscles, mitral annulus, and right ventricular moderator band.
The use of mapping systems predominated (82%); 18% were zero-fluoroscopy procedures. Ablation was preferentially performed with contact forcesensing technology (66.2%), whereas 24.3% used conventional irrigated catheters. Other types of catheters or energy sources were limited (4-mm nonirrigated tip, 4.8%; cryoablation, 0.3%).
There were 25 complications (3.9%): 14 vascular, 10 pericardial effusions, and 1 sedative-induced respiratory acidosis. One death was reported, caused by delayed cardiac tamponade on the ward.
Ventricular tachycardia associated with myocardial infarctionFor this ablation target, 422 procedures were performed in 381 patients. This represents a fall of more than 100 procedures vs 2019, although the number of centers undertaking this type of ablation was largely unchanged (64 vs 66 in 2019). The mean number of procedures/center was 6.6 ± 5.1 (range, 1-22). Most procedures were performed with mapping systems (92%) and with irrigated tip ablation catheters (94.1% in total and 80% with contact forcesensing technology). An increase was seen in the number of zero-fluoroscopy procedures (5%). The overall success rate was 85.3%. Retroaortic access was used in 55.4% and transseptal in 49.8%. The combined endocardial/epicardial approach fell to 11.1%, whereas an exclusively epicardial approach was used in 2.1%.
The main strategy was ablation of the substrate (71.1%). The reported complication rate was 7.3% (similar to that of the previous year): 9 vascular, 7 pericardial effusions, 4 embolic phenomena, 2 atrioventricular blocks, and 1 death of a patient with refractory arrhythmic storm and cardiogenic shock.
Ventricular tachycardia not associated with myocardial infarctionThis ablation target exhibited the lowest drop in the number of procedures, with a total of 247 in 231 patients (19 fewer than in 2019); there was also no change in the number of centers treating this target (n = 51). The mean number of procedures/center was 4.8 ± 4.4 (range, 1-28) and the success rate was 82.6%. This type of ablation was applied to the following ablation targets: nonischemic dilated cardiomyopathy (122 procedures; 84.4% success), arrhythmogenic cardiomyopathy (31 procedures; 81% success); congenital heart diseases (28 procedures; 100% success); hypertrophic cardiomyopathy (13 procedures; 84.6% success); bundle-branch VTs (9 procedures; 100% success); and 29 miscellaneous procedures, which included myocarditis, Chagas disease, valvular heart disease, Brugada syndrome, and noncompaction cardiomyopathy. Retroaortic access was used in 41.3% and transseptal in 31.6%. The exclusively epicardial approach was used in 11.7%, whereas the combined endocardial/epicardial approach was used in 18.6%. Twelve complications were reported (4.9%): 5 pericardial effusions, 2 atrioventricular blocks, 1 vascular, 1 phrenic nerve palsy, 1 pericarditis, and 2 deaths caused by cardiac perforations with tamponade.
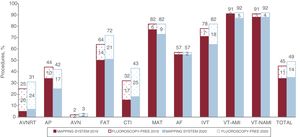
Mapping systems and zero-fluoroscopy ablationIn 2020, almost half of all procedures were performed with mapping system support (7408 procedures; 49%). These systems were most frequently used in VTs in structural heart disease (92%), followed by MAT and IVT (both, 82%). Nonetheless, compared with 2019, the ablation targets showing the greatest proportional increase were CTI (+11%), FAT (+8%), and AVNRT (+6%). In addition, and in line with the trends of previous years, the number of fluoroscopy-free procedures increased again, reaching 2146 (14%). The 3 ablation targets most commonly treated without fluoroscopy were CTI (25%), AVNRT (24%), and FAT (21%). Figure 7 illustrates the proportions of procedures for each ablation target that were conducted with a navigation system or without fluoroscopy.

Percentage of procedures performed with a mapping system and without fluoroscopy in 2019 and 2020. AF, atrial fibrillation; AP, accessory pathway; AVN, atrioventricular node; AVNRT, atrioventricular nodal reentrant tachycardia; CTI, cavotricuspid isthmus; FAT, focal atrial tachycardia; IVT, idiopathic ventricular tachycardia; MAT, macroreentrant atrial tachycardia; VT-AMI, ventricular tachycardia associated with acute myocardial infarction; VT-NAMI, ventricular tachycardia not associated with acute myocardial infarction.
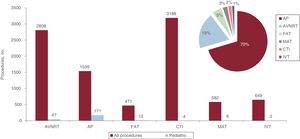
In total, 243 ablations were reported in pediatric patients. This represents a slight increase in the percentage vs the total (1.6%), although the number fell in absolute terms (43 fewer than in 2019). In total, 37 centers reported ablation procedures in pediatric patients (2 fewer than in 2019). However, no center performed more than 50 procedures. One center undertook 44 procedures, whereas another 5 performed between 10 and 20.
APs continue to be the most frequently treated substrate (171 procedures; 70.4%), representing 11.1% of all AP ablations.
AVNRT was the second most frequently treated ablation target (47 procedures; 19.3%), followed by FAT (12 procedures; 4.9%), MAT (6 procedures; 2.5%), CTI (4 procedures; 1.7%), and VTI (3 procedures; 1.2%). Figure 8 shows the distribution by ablation target and as a percentage of the total number of procedures.

Distribution of pediatric procedures by ablation target and as a proportion with respect to the total number of procedures. AP, accessory pathway; AVNRT, atrioventricular nodal reentrant tachycardia; CTI, cavotricuspid isthmus; FAT, focal atrial tachycardia; IVT, idiopathic ventricular tachycardia; MAT, macroreentrant atrial tachycardia.
A total of 80 laboratories (82%) provided specific data on the effects of the pandemic on their clinical practice. In 2020, the laboratories were closed due to the pandemic for an average of 47 ± 33 days. In addition, 72 electrophysiologists (18%) had to self-isolate or were infected with SARS-CoV-2, and 111 SARS-CoV-2-infected patients underwent procedures. The most frequently applied changes to clinical practice included preadmission PCR tests, same-day discharge for simple procedures (in centers that did not do so already), the implementation of shift work, the dedication of a laboratory to SARS-CoV-2 patients in centers with more than 1 available laboratory, and same-day admission (12.5%) or discharge (9%) for complex procedures (only recorded for centers that did not do so before the pandemic). These last 2 measures were largely adopted by high-volume centers.
DISCUSSIONIn 2020, the SARS-CoV-2 pandemic undeniably affected the data reported to the registry. It has had a direct impact on both participation and the number of procedures and the ablation target distribution.
Regarding the fall in the number of procedures, the early days of the pandemic markedly affected high-volume centers, particularly those in large cities, which had to close many of their laboratories for about 2 months, and activity was restricted to emergency procedures, in line with the established recommendations.20 Up to 18% of electrophysiologists were infected or had to self-isolate, with a consequent impact on clinical activity. The centers gradually had to adapt their protocols and working methods and, in addition to the prior PCR screening of patients (which has been almost universal), a widespread effort was made to limit admissions, given the scarcity of available beds, which increased the numbers of outpatient procedures, even for complex patients.
Although there was a reduction in all ablation targets, the greatest impact (particularly due to the volume that it represents) was seen in paroxysmal supraventricular tachycardia procedures, which fell by about 25% vs 2019 and which means that more complex procedures were undertaken overall. This could be one of the reasons why 2020 saw the lowest success rate since 2015. In addition, it is quite likely that the pandemic has meant that patients attending the health care services were more severe or in worse situations (whether due to lower patient referral or even due to fear of infection that compelled patients with less severe conditions to stay at home).
In this regard, the consolidation of AF procedures is notable; despite the pandemic, their number kept increasing proportionally. This is especially relevant given that AF is a supraventricular arrhythmia, with a procedure that has traditionally required hospitalization, and that many centers halted elective procedures for long periods of time in 2020. Although the changes in protocols for admissions and/or discharges in complex procedures have not been universal, they have been adopted by high-volume centers, and we must note that there was no increase in the percentage of complications, which is why many of these changes are probably here to stay, as discussed in the literature.21,22
Regarding AF ablation, we must also stress that, although 2020 showed a slight drop in centers undertaking this procedure, the low activity in a large number of centers continued to be striking. More than half of laboratories performed less than 50 procedures/y, which is not the ideal situation for a complex ablation target. However, many of these low-volume centers are private clinics, whose operators probably also work in the publicly funded health system and accordingly have additional experience. It is also reasonable that centers with less experience would have further reduced their treatment of this substrate in 2020, given that these procedures have traditionally not been conducted in outpatients and, evidently, this type of center decided not to adopt this change in protocol. The coming years will show if this dispersion of procedures remains. Regarding the technique of choice, radiofrequency is still more frequently used than cryoablation, although the latter is nearing 50%. This technique is offered by many of the low-volume centers, probably due to its rapid learning curve.
It is worth mentioning that the pandemic restrictions did not affect the adoption of newer technologies (the use of steerable sheaths and contact forcesensing catheters continued to rise, in pursuit of a higher success rate), and the absence of an effect on the use of mapping systems is particularly striking. The technical support of mapping systems was not only maintained in this highly challenging year, but even showed an increase that cannot a priori be explained by the increased complexity of the ablation targets because it has largely been seen in the supraventricular tachycardias (CTI, FAT, and AVNRT). These 3 substrates are precisely those that were more often treated without fluoroscopy, consolidating the tendency to attempt to avoid ionizing radiation exposure for less complex ablation targets.23
Although the peculiarities of 2020 block direct comparisons, the number of centers performing pediatric ablations continued to fall. Remarkably, none of the centers reached 50 ablations and a major dispersion in the number of cases per center was evident.
Finally, ablation procedures remained a safe technique with a low rate of complications, which has stayed stable over the years. Given that vascular complications were the most frequent complications, they may be a sound target for our efforts. This complication could be minimized by the progressive adoption of ultrasound-guided femoral artery puncture. Although fatal complications remained low in 2020 (0.4%) and all except 1 occurred in complex substrates, the rate of atrioventricular block in AVNRT was 0.2% and there was 1 case of catheter entrapment in the mitral valve that required surgery. Accordingly, our patients must be reminded that all procedures can result in severe complications.
CONCLUSIONSThe Spanish Catheter Ablation Registry has systematically and reliably collected data on the activity and resources of arrhythmia units in Spain for 2 decades. The SARS-CoV-2 pandemic has left its mark, leading to a fall in the number of procedures and a redistribution of ablation targets, with priority given to the most complex substrates. Nonetheless, the overall success rate remained high, with a low rate of complications, and AF became consolidated as the most frequently treated ablation target.
FUNDINGNone.
AUTHORS’ CONTRIBUTIONSAll authors have substantially contributed to the drafting of the original manuscript, the design of the figures, and the final revision. R. Cózar-León has additionally been in charge of data collection and statistical analysis.
CONFLICTS OF INTERESTÓ. Cano Pérez has received fees for consultancy work from Biosense Webster, Medtronic, Boston Scientific, and Biotronik. R. Cózar León has received honoraria from Medtronic, Boston Scientific, and Abbott. I. Anguera Camós has no conflicts of interest.
The coordinators of the registry would once again like to thank all of the participants in the Spanish Catheter Ablation Registry (appendix 1), whose selfless help every year permit the publication of this document. Our thanks must also go to Cristina Plaza for her invaluable work.
Jesús Almendral-Garrote, Pau Alonso-Fernández, Concepción Alonso-Martín, Nelson María Alvarenga-Recalde, Luis Álvarez-Acosta, Miguel Álvarez-López, Ignasi Anguera-Camós, Eduardo Arana-Rueda, Álvaro Arce-León, María Fe Arcocha-Torres, Miguel Ángel Arias-Palomares, Antonio Asso-Abadía, Gabriel Ballesteros-Derbenti, Alberto Barrera-Cordero, Pablo Bastos-Amador, Juan Benezet-Mazuecos, Bruno Bochard-Villanueva, Andrés I. Bodegas-Cañas, María del Pilar Cabanas-Grandío, Lucas R. Cano-Calabria, Antonio J. Cartón-Sánchez, Silvia del Castillo-Arrojo, Víctor Castro-Urda, Rocío Cózar-León, Ernesto Díaz-Infante, Juan Manuel Durán-Guerrero, Juliana Elices-Teja, María del Carmen Expósito-Pineda, Juan Manuel Fernández-Gómez, José Ferrando-Cervelló, Julio Jesús Ferrer-Hita, María Luisa Fidalgo-Andrés, Adolfo Fontenla-Cerezuela, Arcadio García-Alberola, Enrique García-Cuenca, Francisco Javier García-Fernández, Ignacio Gil-Ortega, Federico Gómez-Pulido, Eduard Guasch-i-Casany, José M. Guerra-Ramos, Benito Herreros-Guilarte, Víctor Manuel Hidalgo-Olivares, Alicia Ibáñez-Criado, José Luis Ibáñez-Criado, Sonia Ibars-Campaña, F. Javier Jiménez-Candil, Jesús I. Jiménez-López, Carla Lázaro-Rivera, José Miguel Lozano-Herrera, Ángel Martínez-Brotons, José Luis Martínez-Sande, Gabriel Martín-Sánchez, Roberto Matías-Francés, Francisco Mazuelos-Bellido, Elena Mejía-Martínez, Diego Menéndez-Ramírez, José Luis Merino-Llorens, Josep Lluis Mont-Girbau, José Moreno-Arribas, Javier Moreno-Planas, Pablo Moriña-Vázquez, Ángel Moya-i-Mitjans, Josep Navarro-Manchón, Joaquín Osca-Asensi, Agustín Pastor-Fuentes, Ricardo Pavón-Jiménez, Rafael Peinado-Peinado, Luisa Pérez-Álvarez, Nicasio Pérez-Castellano, Andreu Porta-Sánchez, Jordi Punti-Sala, Aurelio Quesada-Dorador, Pablo Ramos Ardanaz, Javier Ramos-Maqueda, Nuria Rivas-Gándara, Felipe José Rodríguez-Entem, Enrique Rodríguez-Font, Juan Carlos Rodríguez-Pérez, Rafael Romero-Garrido, José Manuel Rubín-López, Amador Rubio-Caballero, José Manuel Rubio-Campal, Pablo M. Ruiz-Hernández, Ricardo Salgado-Aranda, María de Gracia Sandín-Fuentes, Axel Sarrias-Mercé, Alba Santos-Ortega, Jose María Segura-Saint-Gerons, Federico Segura-Villalobos, and Irene Valverde-André.
| Andalusia | |
| Cádiz | Hospital Universitario Puerta del Mar (Lucas R. Cano-Calabria) |
| Granada | Hospital Universitario Virgen de las Nieves (Miguel Álvarez-López); Hospital Clínico Universitario San Cecilio (José Miguel Lozano-Herrera) |
| Huelva | Hospital Juan Ramón Jiménez, Hospital Quirón Huelva (Pablo Moriña Vázquez) |
| Córdoba | Hospital Universitario Reina Sofía (Jose María Segura-Saint-Gerons/Francisco Mazuelos-Bellido) |
| Málaga | Hospital Clínico Universitario Virgen de la Victoria, Hospital Vithas Xanit Internacional Benalmádena, Hospital Vithas Málaga Parque San Antonio, Hospital Quirón Salud Málaga, Hospital Quirón Salud Marbella (Alberto Barrera-Cordero); Hospital Regional Universitario de Málaga, Hospital HLA El Ángel (Gabriel Ballesteros-Derbenti) |
| Sevilla | Hospital Universitario Virgen Macarena (Rocío Cózar-León, Pablo Bastos-Amador); Hospital Vithas Sevilla (Ernesto Díaz-Infante); Hospital Universitario Virgen del Rocío (Eduardo Arana Rueda); Hospital Universitario Virgen de Valme (Ricardo Pavón-Jiménez); Hospital Quirón Salud Infanta Luisa (Rafael Romero-Garrido); Hospital Quirón Salud Sagrado Corazón (Juan Manuel Fernández-Gómez); Hospital HLA Santa Isabel (Álvaro Arce León) |
| Aragon | |
| Zaragoza | Hospital Universitario Miguel Servet, Hospital Quirónsalud Zaragoza (Antonio Asso-Abadía); Hospital Clínico Universitario Lozano Blesa (Javier Ramos-Maqueda) |
| Principality of Asturias | Hospital Universitario de Cabueñes (Irene Valverde-André); Hospital Universitario Central de Asturias (José Manuel Rubín-López) |
| Balearic Islands | Hospital Universitario Son Espases (María del Carmen Expósito-Pineda); Clínica Rotger Quirón, Hospital Quirónsalud Palmaplanas (Nelson M. Alvarenga-Recalde) |
| Canary Islands | |
| Las Palmas | Hospital Vithas Santa Catalina (Juan Carlos Rodríguez-Pérez); Hospital Perpetuo Socorro (Pablo M. Ruiz-Hernández); Hospital Universitario Insular de Gran Canaria (Federico Segura-Villalobos) |
| Santa Cruz de Tenerife | Hospital Universitario Nuestra Señora de la Candelaria, Hospital San Juan de Dios Tenerife (Luis Álvarez-Acosta); Complejo Hospitalario Universitario de Canarias (Julio Jesús Ferrer-Hita) |
| Cantabria | Hospital Universitario Marqués de Valdecilla (Felipe José Rodríguez Entem) |
| Castile-La Mancha | |
| Toledo | Complejo Hospitalario Universitario de Toledo (Miguel Ángel Arias-Palomares) |
| Albacete | Hospital General Universitario de Albacete (Víctor M. Hidalgo-Olivares) |
| Castile and León | |
| Burgos | Hospital Universitario de Burgos (F. Javier García Fernández) |
| León | Complejo Asistencial Universitario de León (María Luisa Fidalgo-Andrés) |
| Salamanca | Complejo Asistencial Universitario de Salamanca (F. Javier Jiménez-Candil) |
| Valladolid | Hospital Clínico Universitario de Valladolid (María de Gracia Sandín-Fuentes); Hospital Universitario Río Hortega (Benito Herreros-Guilarte) |
| Catalonia | |
| Barcelona | Hospital Universitario de Bellvitge (Ignasi Anguera-Camós); Hospital Clínic (Eduard Guasch-i-Casany, Josep Lluís Mont-Girbau); Hospital Universitario Germans Trias i Pujol (Axel Sarrias-Mercé); Hospital Universitario Vall d’Hebron (Nuria Rivas-Gándara, Alba Santos-Ortega); Clínica Corachán (José M. Guerra-Ramos); Clínica Sagrada Família, Hospital Universitario Dexeus (Ángel Moya-i-Mitjans); Hospital Universitario Mútua de Terrassa (Sonia Ibars-Campaña); Hospital del Mar (Jesús I. Jiménez-López); Hospital Universitario Parc Taulí de Sabadell (Jordi Punti-Sala); Hospital de la Santa Creu y Sant Pau (Concepción Alonso-Martín); Clínica Teknon (Enrique Rodríguez-Font) |
| Tarragona | Hospital Universitario Joan XXIII (Gabriel Martín Sánchez) |
| Lleida | Hospital Universitario Arnau de Vilanova (Diego-Menéndez-Ramírez) |
| Valencian Community | |
| Alicante | Hospital Universitario San Juan de Alicante (José Moreno-Arribas); Hospital General Universitario de Alicante (José Luis Ibáñez-Criado); Cardioritmo Levante (Alicia Ibáñez-Criado) |
| Castellón | Hospital General Universitario de Castellón (Josep Navarro-Manchón) |
| Valencia | Hospital General Universitario de Valencia (Aurelio Quesada-Dorador); Hospital Universitario y Politécnico La Fe (Joaquín Osca-Asensi); Hospital Clínico Universitario de Valencia (Ángel Martínez-Brotons); Hospital de Manises (Pau Alonso-Fernández); Hospital Universitario de la Ribera (Bruno Bochard-Villanueva); Hospital Universitario Dr. Peset (José Ferrando-Cervelló) |
| Extremadura | |
| Badajoz | Hospital Universitario de Badajoz (Juan Manuel Durán-Guerrero) |
| Galicia | |
| A Coruña | Hospital Universitario de A Coruña (Luisa Pérez-Álvarez); Hospital Clínico Universitario de Santiago de Compostela (José Luis Martínez-Sande) |
| Pontevedra | Hospital Álvaro Cunqueiro (María del Pilar Cabanas-Grandío) |
| Lugo | Hospital Universitario Lucus Augusti (Juliana Elices-Teja) |
| Community of Madrid | Hospital Universitario Ramón y Cajal (Javier Moreno-Planas); Hospital Sanitas La Moraleja (Roberto Matías-Francés); Hospital Universitario 12 de Octubre (Adolfo Fontenla-Cerezuela); Hospital Universitario de Getafe (Agustín Pastor-Fuentes); HM Hospitales (Jesús Almendral-Garrote); Hospital Universitario Puerta de Hierro (Víctor Castro-Urda); Hospital Universitario La Paz (Rafael Peinado-Peinado); Hospital Universitario La Paz-Unidad de Electrofisiología Robotizada (José Luis Merino-Llorens); Hospital Vithas Madrid Aravaca (José Luis Merino-Llorens); Hospital Ruber Juan Bravo/Hospital Universitario Quirónsalud Madrid (Andreu Porta-Sánchez/José Luis Merino-Llorens); Hospital Universitario La Paz-Infantil (Antonio J. Cartón-Sánchez, José Luis Merino-Llorens); Hospital Clínico San Carlos (Nicasio Pérez Castellano); Hospital Universitario Fundación Alcorcón (Amador Rubio-Caballero); Hospital Universitario Fundación Jiménez Díaz (José Manuel Rubio-Campal); Hospital Universitario Severo Ochoa (Ricardo Salgado-Aranda); Hospital Quirón La Luz (Juan Benezet-Mazuecos); Hospital Universitario Rey Juan Carlos (Federico Gómez-Pulido/Elena Mejía); Hospital Universitario de Torrejón (Carla Lázaro-Rivera); Hospital Universitario de Fuenlabrada (Silvia del Castillo-Arrojo) |
| Region of Murcia | Hospital Universitario Virgen de la Arrixaca (Arcadio García-Alberola); Hospital General Universitario Santa Lucía (Ignacio Gil-Ortega) |
| Chartered Community of Navarre | Clínica Universidad de Navarra (Pablo Ramos-Ardanaz) |
| Basque Country | |
| Álava | Hospital Universitario Txagorritxu (Enrique García-Cuenca) |
| Vizcaya | Hospital de Cruces (Andrés I. Bodegas-Cañas); Hospital de Basurto (María Fe Arcocha-Torres) |
| La Rioja | Hospital Viamed Los Manzanos (Francisco Javier García-Fernández) |