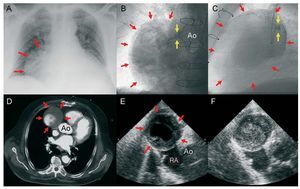
A 73-year-old man who had undergone coronary artery bypass surgery 13 years previously (mammary to left anterior descending artery and saphenous to the second diagonal, obtuse marginal, and posterior descending arteries) was referred for an inferior ST-segment elevation myocardial infarction. Chest radiography disclosed an image occupying a part of the right hemithorax (Figure, A, red arrows). Coronary angiography showed no changes in the lesions of the native vessels and the mammary bypass was patent. During the attempts to canalize the saphenous grafts, contrast injection to the interior of an aortic pseudoaneurysm occurred (red arrows in Figure, B, posteroanterior view and Figure, C, left lateral view). The pseudoaneurysm was 75´55 mm in size, had a mural thrombus, and communicated with the ascending aorta through a narrow anastomotic opening located in the right anterolateral wall (yellow arrows). Chest computed tomography (Figure, D) and echocardiography (Figure, E, right parasternal view) confirmed an anterolateral location with respect to the aorta (Ao) and right atrium (RA). Doppler study demonstrated weak bidirectional flow through the mouth of the pseudoaneurysm. None of the saphenous grafts were patent and the pseudoaneurysm was considered to derive from the proximal anastomosis of the bypass to the posterior descending artery. Conservative management was applied in the acute phase, and although surgery was planned, serial imaging studies revealed progressive thrombosis of the pseudoaneurysm cavity (Figure, F). Unfortunately, the patient died from a pneumonic process before the procedure could be carried out.

Figure.