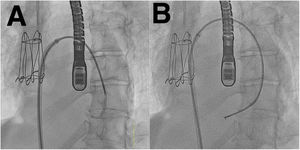
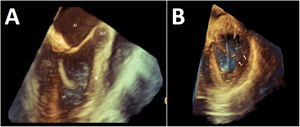

In the assessment of a 49-year-old woman with cardiomyopathy, cardiac magnetic resonance showed patchy late enhancement predominantly in the anterior interventricular septum (IVS); endomyocardial biopsy (EMB) of the right ventricle was inconclusive. The left ventricle (LV) was mildly dilated with an ejection fraction of 35% and moderate-severe secondary mitral regurgitation (MR). Following several admissions for heart failure, it was decided to treat the MR percutaneously. Taking advantage of the transseptal access and 3D transesophageal echocardiogram (TEE) used in the mitral repair, an EMB of the LV was performed in the same procedure. Via the sheath introducer that was used in the transseptal puncture and located in the left atrium, a coronary catheter (Judkins right) was introduced into the LV. Under fluoroscopic guidance, the catheter was directed toward the IVS (figure 1A), a 104cm bioptome (CardinalHealth, USA) was advanced, and 5 samples were taken (figure 1B; ). The 3D TEE (figure 2A; ) allowed the catheter to be guided more precisely toward the most affected area of the LV (anterior IVS, asterisk). Before each sample, TEE was used to confirm (figure 2B) that the bioptome was facing the anterior IVS (asterisk), avoiding the more basal septum and away from the mitral subvalvular apparatus (arrows). There were no recorded abnormalities of the conduction system. After the EMB, an NTW clip (Abbott, USA) was implanted, leaving mild residual MR. Usually, EBM of the LV is done via a retrograde transaortic approach; with echocardiographic guidance, the transseptal approach appears to be a feasible alternative for biopsy of the different walls of the LV. The patient gave consent for this publication.
FUNDING

None.
AUTHORS’ CONTRIBUTIONSAll authors participated in the design, writing, and review of the final article.
CONFLICTS OF INTERESTThe authors have no conflicts of interest relating to this article.
Supplementary data associated with this article can be found in the online version, at https://doi.org/10.1016/j.rec.2021.12.009