
A 62-year-old woman with a 3-year history of chest pain underwent transthoracic echocardiography that revealed asymmetric septal hypertrophy, no systolic anterior motion, mildly dilatated left atrium (LA), and left ventricular systolic function of 69%.
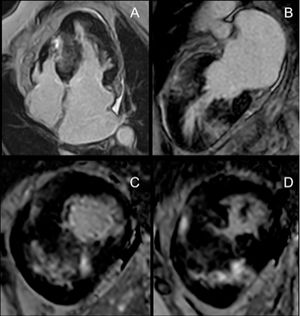
Cardiac magnetic resonance imaging confirmed septal hypertrophy (30.8mm in the midseptum). Right ventricular hypertrophy and delayed enhancement with nonischemic pattern were also observed (figure 1). The risk of sudden cardiac death was calculated as 2.2% and, therefore, she was not eligible for an implantable cardiac defibrillator.

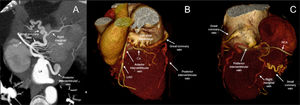
Cardiac tomography reported normal coronary arteries, but showed that the great coronary vein, posterior interventricular vein, and small coronary vein ended directly at the LA. There was no evidence of coronary sinus (CS) or left superior vena cava (figure 2; RCA, right coronary artery; Cx, circumflex artery; LAD, left anterior descending artery).

Absence of the CS together with hypertrophic cardiomyopathy is very rare; hence, informed consent was obtained from the patient for publication.
Familiarity with congenital anomalies of the CS and the coronary veins is essential when planning some cardiac surgical procedures and repair surgeries for associated cardiac lesions. Absence of the CS is usually divided into the presence or absence of persistent left superior vena cava. In our patient, direct cardiac venous drainage into the LA produces small right-to-left shunting with minimal hemodynamic repercussions.
FUNDINGNone.
AUTHORS’ CONTRIBUTIONSD.I. Katekaru-Tokeshi compiled the data, interpreted the cardiac tomography images, and wrote the article. K. Menacho interpreted the cardiac magnetic resonance images and provided a critical review of the article. M. Jiménez-Santos provided a critical review of the article. All authors approved the final version.
CONFLICTS OF INTERESTNone declared.