
Left ventricular hypertrabeculation/noncompaction (LVHT) is a cardiac abnormality of unknown etiology. Usually the myocardial trabeculations in LVHT are covered with endocardium, but fibrosis, endocardial thickening, and fibroelastosis have been also reported. LVHT may be associated with several extracardiac disorders including neuromuscular disorders. LVHT associated with immune deficiency has been reported only in Roifman syndrome.
In a 47-year old patient with recurrent infections since early childhood and heart failure, left ventricular hypertrabeculation/noncompaction (LVHT) was diagnosed echocardiographically. Laboratory investigations disclosed a mannose-binding leptin (MBL) of 18 ng/mL (normal: 60-5500). Neurological investigation revealed ptosis, reduced tendon reflexes, warming-up phenomenon, and a myogenic electromyogram. Muscle biopsy from the pectoralis muscle showed slight fiber size variation, some moderately atrophic fibers, occasionally regenerating fibers, slight irregularities of the oxidative enzymes, type-II -fiber predominance, and some rimmed vacuoles. Myopathy of unknown etiology was diagnosed. Despite implantation of a cardiac defibrillator and biventricular pacing system, he died due to pneumonia complicated by renal failure and hepatic failure.
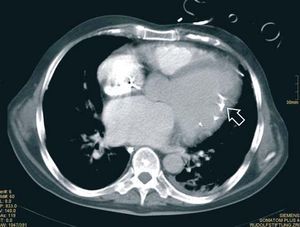
LVHT was confirmed by autopsy (Figure 1, left). In contrast to previously described autoptic and histological investigations of LVHT, the patient showed extensive endocardial calcifications (Figure 1, left, arrow), including the hypertrabeculated myocardium. These calcifications were also visible on cardiac computed tomography (Figure 2, right). The endocardial calcifications were interpreted as a result of recurrent endocarditic episodes in the immunocompromised patient, promoted by the MBL deficiency. Altered left ventricular blood flow mechanisms within the trabecular meshwork of LVHT may have additionally favoured the adherence of bacteria and consequently development of infections.

Figure 1.

Figure 2.