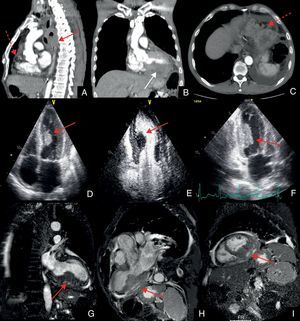
A 56-year-old male with a 4 pack-year smoking history was admitted after an episode of syncope. The patient reported 2 months of fatigue, exertional dyspnea, pleuritic chest pain, and 10-kilogram weight loss. Physical examination was remarkable for paleness, and blood count revealed anemia of 7.2g/dL. Endoscopy showed an ulcero-vegetating tumor in the mid-esophagus and histological examination revealed an invasive squamous cell carcinoma. Computed tomography (Fig. A-C) showed extensive thickening of the mid-esophagus with a mass extending to the surrounding mediastinum (red straight arrow), up to the aortic arch and down to the pulmonary veins. Metastatic nodules (dotted arrows) and a larger mass evolving the inferolateral region of the left ventricle could be seen (white straight arrow). Echocardiogram demonstrated the infiltrative mass in the left ventricle (Fig. D-F, arrows), extending intracavitary and causing outflow tract turbulence but no significant gradient. Cardiac magnetic resonance imaging confirmed the extensive infiltrating myocardial mass and pericardial thickness with solid formations (Fig. G-I, arrows). Since the patient was clinically stable it was decided to discharge him to home with a scheduled oncology evaluation. Unfortunately he was admitted 4 days later in emergency care with hospital acquired pneumonia and died due to acute respiratory failure.

Cardiac metastasis of tumors arising from the esophagus are rare and particularly uncommon if caused by squamous cell carcinoma. This is usually associated with poor prognosis and most therapies are palliative. This case illustrates an unusual clinical presentation of esophageal tumor with cardiac invasion.