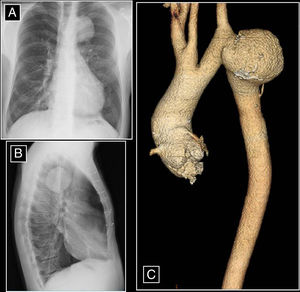
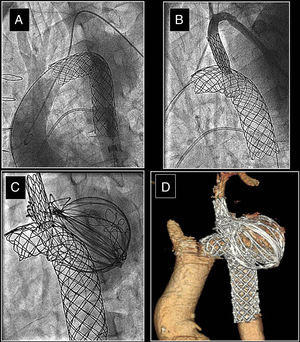
A 43-year-old man was diagnosed at birth with a severe aortic coarctation that was surgically treated in infancy. He had a favorable clinical course, normal growth, and no evidence of heart failure. However, at the age of 7 years, he was diagnosed with restenosis of the coarctation and mild subaortic membrane stenosis. At the age of 9 years, the patient underwent surgery for the recoarctation, with resection of the recoarctated segment and an end-to-end anastomosis. At the age of 11 years, he required a new surgical intervention to treat the subaortic membrane stenosis, which had progressed to a severe state. The patient had a good clinical course and stopped attending successive follow-up visits until, at the age of 43 years, a routine chest radiograph showed a huge aneurysm in the aortic arch. The chest plain film and computed tomography image before the intervention are shown in Figure 1. A “tailor-made” covered stent (135mm length × 20mm diameter) was ordered and implanted in the aorta in an attempt to exclude the aneurysm (Figure 2A). By perforating the synthetic material from the left subclavian artery with a metal guidewire captured in the aorta, blood flow toward the subclavian was re-established. A new covered stent was implanted in the origin (8 × 34mm; Figure 2B). The aneurysm was partially excluded and thrombosed, but a small leak persisted. At 1 year following the procedure, the residual cavity was probed and filled with coils and teflon-covered metal wires, which achieved complete exclusion of the aneurysm (Figure 2C,D).
ISSN: 1885-5857
Impact factor 2024
4.9

